Markey Cancer Center, University of Kentucky, Lexington.
Division of Cancer Biostatistics, College of Medicine, University of Kentucky, Lexington.
JAMA Oncol. 2024 Apr 1;10(4):500-507. doi: 10.1001/jamaoncol.2023.6969.
The COVID-19 pandemic disrupted the normal course of cancer screening and detection in the US. A nationwide analysis of the extent of this disruption using cancer registry data has not been conducted.
To assess the observed and expected cancer rate trends for March through December 2020 using data from all 50 US states and the District of Columbia.
DESIGN, SETTINGS, AND PARTICIPANTS: This was a population-based cross-sectional analysis of cancer incidence trends using data on cases of invasive cancer diagnosis reported to the US Cancer Statistics from January 1, 2018, through December 31, 2020. Data analyses were performed from July 6 to 28, 2023.
EXPOSURE(S): Age, sex, race, urbanicity, and state-level response to the COVID-19 pandemic at the time of cancer diagnosis.
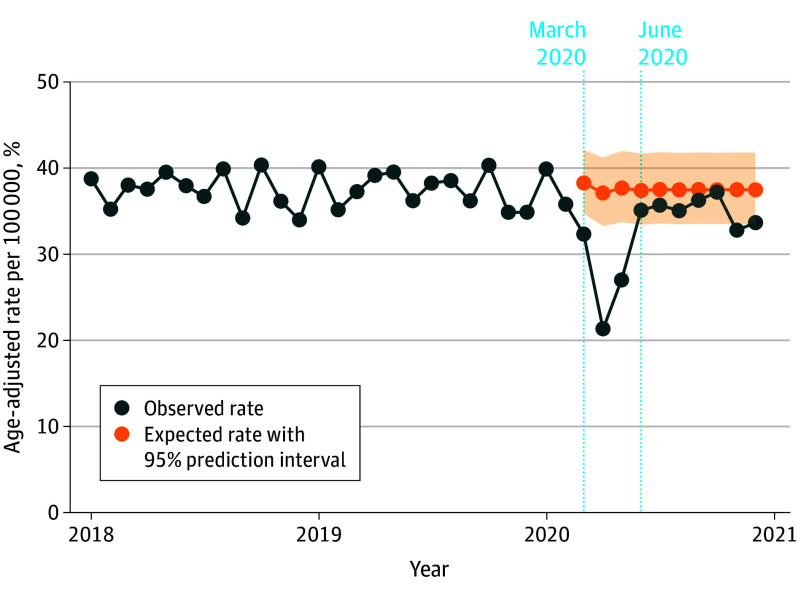
Used time-series forecasting methods to calculate expected cancer incidence rates for March 1 through December 31, 2020, from prepandemic trends (January 2018-February 2020). Measured relative difference between observed and expected cancer incidence rates and numbers of potentially missed cancer cases.
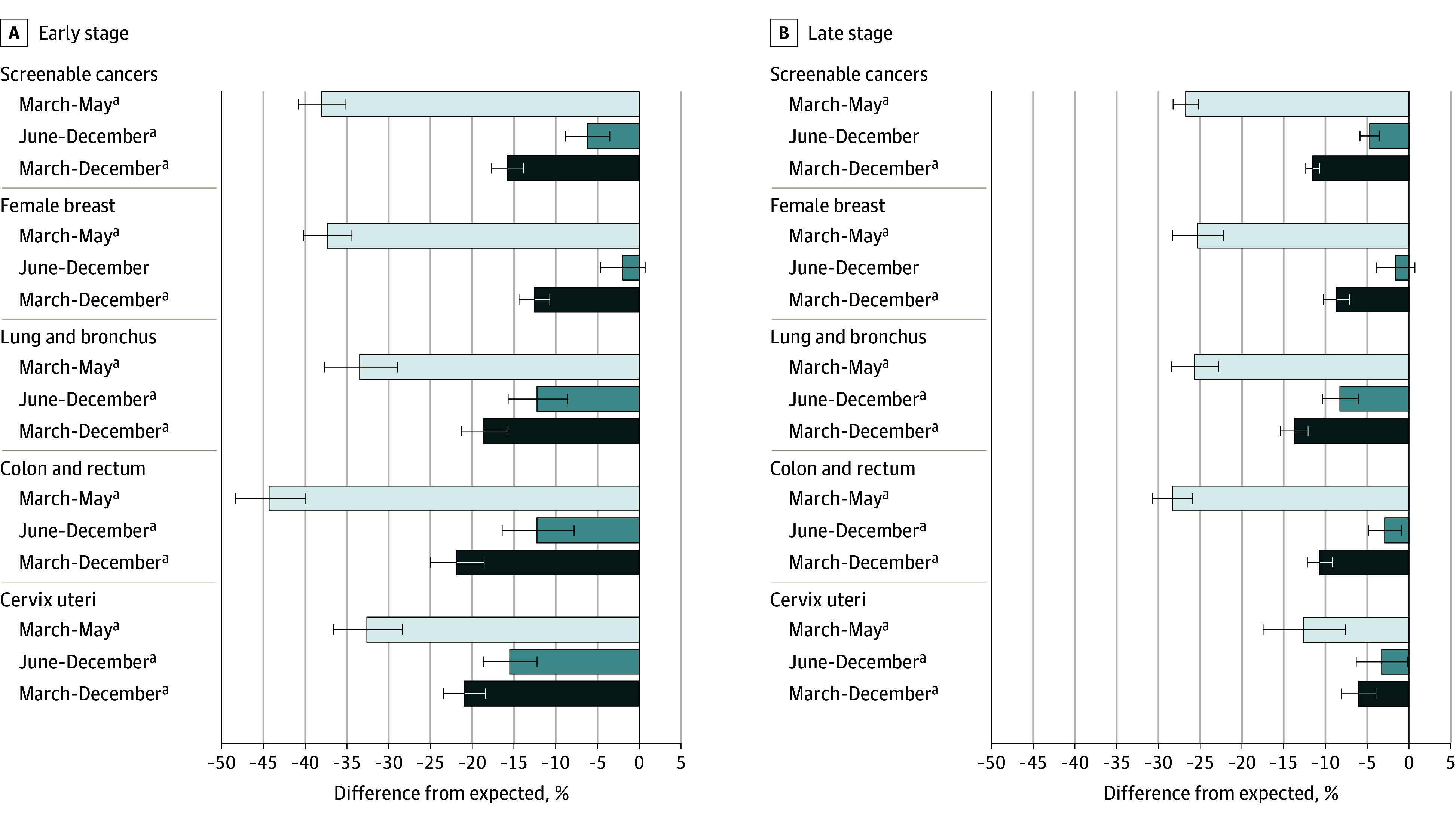
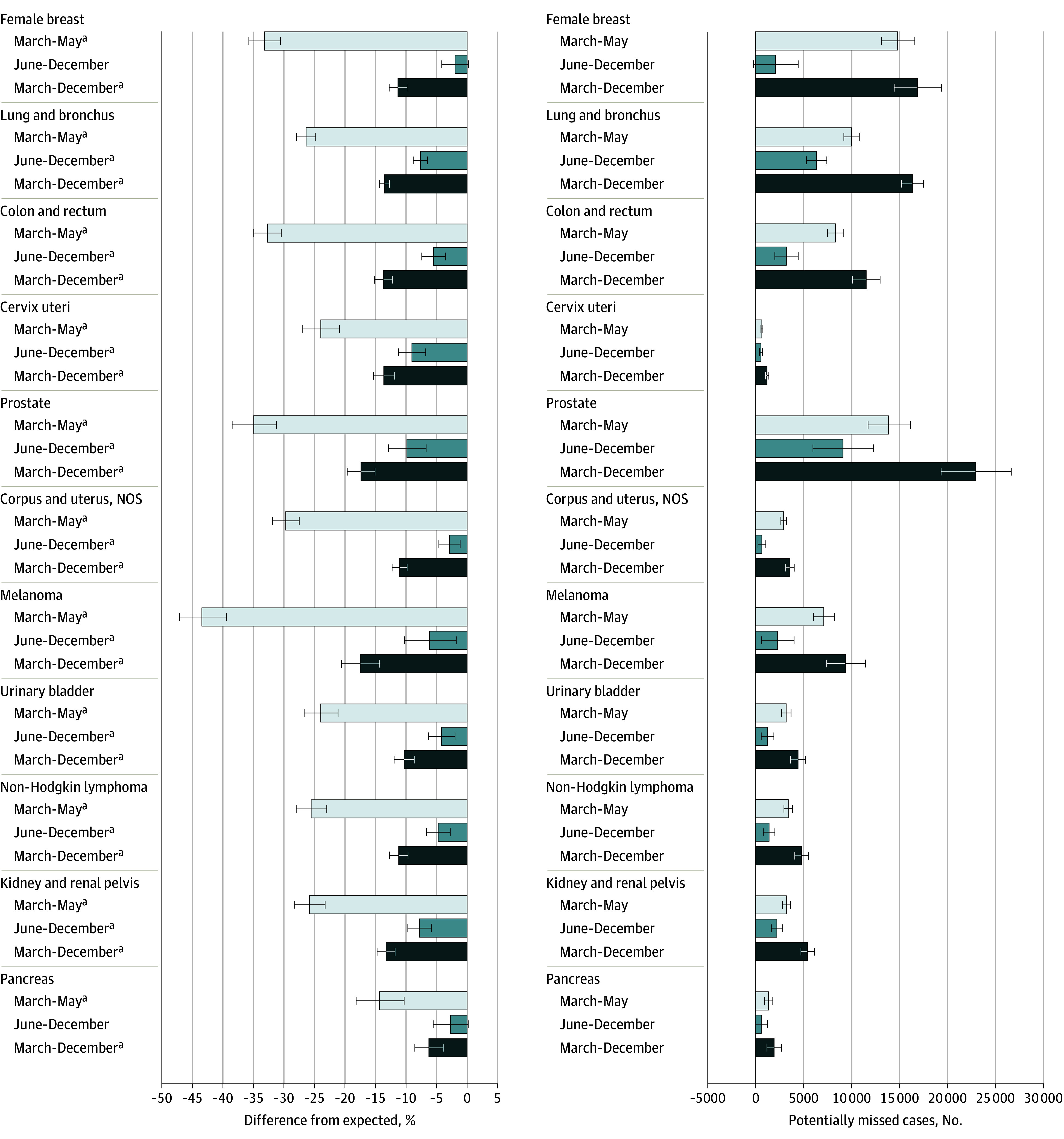
This study included 1 297 874 cancer cases reported in the US from March 1 through December 31, 2020, with an age-adjusted incidence rate of 326.5 cases per 100 000 population. Of the observed cases, 657 743 (50.7%) occurred in male patients, 757 106 (58.3%) in persons 65 years or older, and 1 066 566 (82.2%) in White individuals. Observed rates of all-sites cancer incidence in the US were 28.6% (95% prediction interval [PI], 25.4%-31.7%) lower than expected during the height of the COVID-19 pandemic response (March-May 2020); 6.3% (95% PI, 3.8%-8.8%) lower in June to December 2020; and overall, 13.0% (95% PI, 11.2%-14.9%) lower during the first 10 months of the pandemic. These differences indicate that there were potentially 134 395 (95% PI, 112 544-156 680) undiagnosed cancers during that time frame. Prostate cancer accounted for the largest number of potentially missed cases (22 950), followed by female breast (16 870) and lung (16 333) cancers. Screenable cancers saw a total rate reduction of 13.9% (95% PI, 12.2%-15.6%) compared with the expected rate. The rate of female breast cancer showed evidence of recovery to previous trends after the first 3 months of the pandemic, but levels remained low for colorectal, cervical, and lung cancers. From March to May 2020, states with more restrictive COVID-19 responses had significantly greater disruptions, yet by December 2020, these differences were nonsignificant for all sites except lung, kidney, and pancreatic cancer.
This cross-sectional analysis of cancer incidence trends found a substantial disruption to cancer diagnoses in the US during the first 10 months of the COVID-19 pandemic. The overall and differential findings can be used to inform where the US health care system should be looking to make up ground in cancer screening and detection.
COVID-19 大流行扰乱了美国的癌症筛查和检测的正常进程。使用癌症登记数据对这种干扰的程度进行的全国性分析尚未进行。
使用来自美国所有 50 个州和哥伦比亚特区的数据,评估 2020 年 3 月至 12 月期间观察到和预期的癌症发病率趋势。
设计、设置和参与者:这是一项基于人群的癌症发病率趋势的横断面分析,使用的是 2018 年 1 月 1 日至 2020 年 12 月 31 日期间报告给美国癌症统计数据的侵袭性癌症诊断病例的数据。数据分析于 2023 年 7 月 6 日至 28 日进行。
癌症诊断时的年龄、性别、种族、城市性和州级对 COVID-19 大流行的反应。
使用时间序列预测方法,根据大流行前的趋势(2018 年 1 月至 2020 年 2 月)计算 2020 年 3 月 1 日至 12 月 31 日的预期癌症发病率。测量观察到的和预期的癌症发病率之间的相对差异,以及潜在错过的癌症病例的数量。
这项研究包括 2020 年 3 月 1 日至 12 月 31 日期间在美国报告的 1297874 例癌症病例,年龄调整后的发病率为每 100000 人 326.5 例。观察到的病例中,657743 例(50.7%)发生在男性患者中,757106 例(58.3%)发生在 65 岁或以上的人群中,1066566 例(82.2%)发生在白人个体中。在 COVID-19 大流行应对的高峰期(2020 年 3 月至 5 月),美国所有部位癌症的观察发病率比预期低 28.6%(95%预测区间[PI],25.4%-31.7%);6.3%(95%PI,3.8%-8.8%)在 6 月至 12 月 2020 年较低;总体而言,在大流行的前 10 个月内,发病率低 13.0%(95%PI,11.2%-14.9%)。这些差异表明,在此期间可能有 134395 例(95%PI,112544-156680)癌症未被诊断。前列腺癌占潜在漏诊病例的最大数量(22950 例),其次是女性乳腺癌(16870 例)和肺癌(16333 例)。与预期相比,可筛查癌症的总发病率下降了 13.9%(95%PI,12.2%-15.6%)。在 COVID-19 大流行的前 3 个月后,女性乳腺癌的发病率显示出恢复到以前趋势的迹象,但结直肠癌、宫颈癌和肺癌的发病率仍然较低。从 2020 年 3 月至 5 月,COVID-19 反应较为严格的州的干扰明显更大,但到 2020 年 12 月,除肺癌、肾脏和胰腺外,所有部位的差异均不显著。
这项癌症发病率趋势的横断面分析发现,在美国 COVID-19 大流行的前 10 个月期间,癌症诊断受到了严重干扰。总体和差异发现可以用来告知美国医疗保健系统应该在哪里寻找弥补癌症筛查和检测的机会。