Băghină Ruxandra-Maria, Crișan Simina, Luca Silvia, Pătru Oana, Lazăr Mihai-Andrei, Văcărescu Cristina, Negru Alina Gabriela, Luca Constantin-Tudor, Gaiță Dan
Cardiology Department, "Victor Babes" University of Medicine and Pharmacy, 2 Eftimie Murgu Sq., 300041 Timisoara, Romania.
Institute of Cardiovascular Diseases Timisoara, 13A Gheorghe Adam Street, 300310 Timisoara, Romania.
J Clin Med. 2024 Aug 27;13(17):5088. doi: 10.3390/jcm13175088.
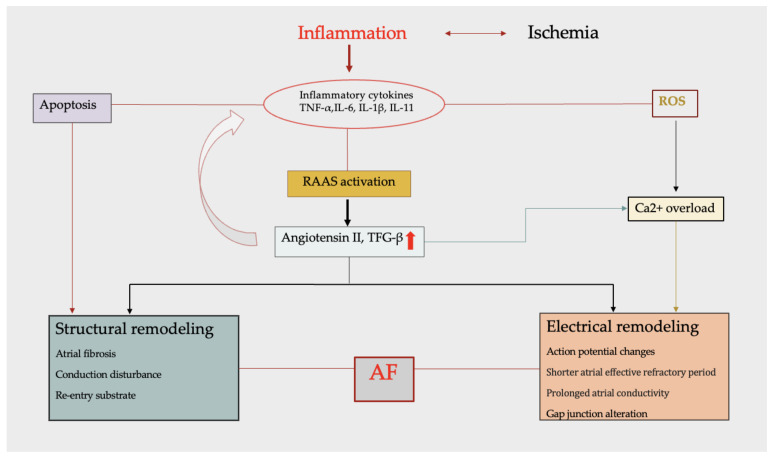
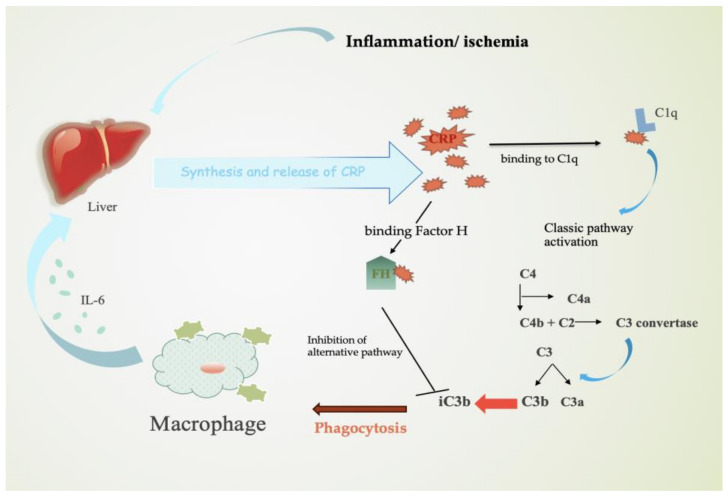
Acute coronary syndrome (ACS) is a complex clinical syndrome that encompasses acute myocardial infarction (AMI) and unstable angina (UA). Its underlying mechanism refers to coronary plaque disruption, with consequent platelet aggregation and thrombosis. Inflammation plays an important role in the progression of atherosclerosis by mediating the removal of necrotic tissue following myocardial infarction and shaping the repair processes that are essential for the recovery process after ACS. As a chronic inflammatory disorder, atherosclerosis is characterized by dysfunctional immune inflammation involving interactions between immune (macrophages, T lymphocytes, and monocytes) and vascular cells (endothelial cells and smooth muscle cells). New-onset atrial fibrillation (NOAF) is one of the most common arrhythmic complications in the setting of acute coronary syndromes, especially in the early stages, when the myocardial inflammatory reaction is at its maximum. The main changes in the atrial substrate are due to atrial ischemia and acute infarcts that can be attributed to neurohormonal factors. The high incidence of atrial fibrillation (AF) post-myocardial infarction may be secondary to inflammation. Inflammatory response and immune system cells have been involved in the initiation and development of atrial fibrillation. Several inflammatory indexes, such as C-reactive protein and interleukins, have been demonstrated to be predictive of prognosis in patients with ACS. The cell signaling activation patterns associated with fibrosis, apoptosis, and hypertrophy are forms of cardiac remodeling that occur at the atrial level, predisposing to AF. According to a recent study, the presence of fibrosis and lymphomononuclear infiltration in the atrial tissue was associated with a prior history of AF. However, inflammation may contribute to both the occurrence/maintenance of AF and its thromboembolic complications.
急性冠状动脉综合征(ACS)是一种复杂的临床综合征,包括急性心肌梗死(AMI)和不稳定型心绞痛(UA)。其潜在机制是冠状动脉斑块破裂,继而导致血小板聚集和血栓形成。炎症在动脉粥样硬化进展中起重要作用,它介导心肌梗死后坏死组织的清除,并塑造ACS后恢复过程所必需的修复过程。作为一种慢性炎症性疾病,动脉粥样硬化的特征是免疫炎症功能失调,涉及免疫细胞(巨噬细胞、T淋巴细胞和单核细胞)与血管细胞(内皮细胞和平滑肌细胞)之间的相互作用。新发房颤(NOAF)是急性冠状动脉综合征最常见的心律失常并发症之一,尤其是在早期,此时心肌炎症反应最为强烈。心房基质的主要变化是由于心房缺血和急性梗死,这可归因于神经激素因素。心肌梗死后房颤(AF)的高发病率可能继发于炎症。炎症反应和免疫系统细胞参与了房颤的发生和发展。一些炎症指标,如C反应蛋白和白细胞介素,已被证明可预测ACS患者的预后。与纤维化、凋亡和肥大相关的细胞信号激活模式是心房水平发生的心脏重塑形式,易导致房颤。根据最近的一项研究,心房组织中纤维化和淋巴细胞单核细胞浸润的存在与房颤病史有关。然而,炎症可能促成房颤的发生/维持及其血栓栓塞并发症。