The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, 310053, People's Republic of China.
Heart Center, Department of Cardiovascular Medicine, Zhejiang Provincial People's Hospital (Affiliated People's Hospital), Hangzhou Medical College, Hangzhou, Zhejiang, China.
BMC Cardiovasc Disord. 2023 Sep 1;23(1):432. doi: 10.1186/s12872-023-03480-9.
New-onset atrial fibrillation (NOAF) is a common adverse outcome of percutaneous coronary intervention (PCI) in patients with acute myocardial infarction (AMI) and is closely correlated with hospital stay and prognosis. In recent years, serum fibrinogen-to-albumin ratio (FAR), a novel biomarker for inflammation and thrombosis, has been used to predict the severity and prognosis of coronary artery disease. Our study aimed to investigate the relationship between FAR and NOAF during hospitalization after PCI in patients with AMI.
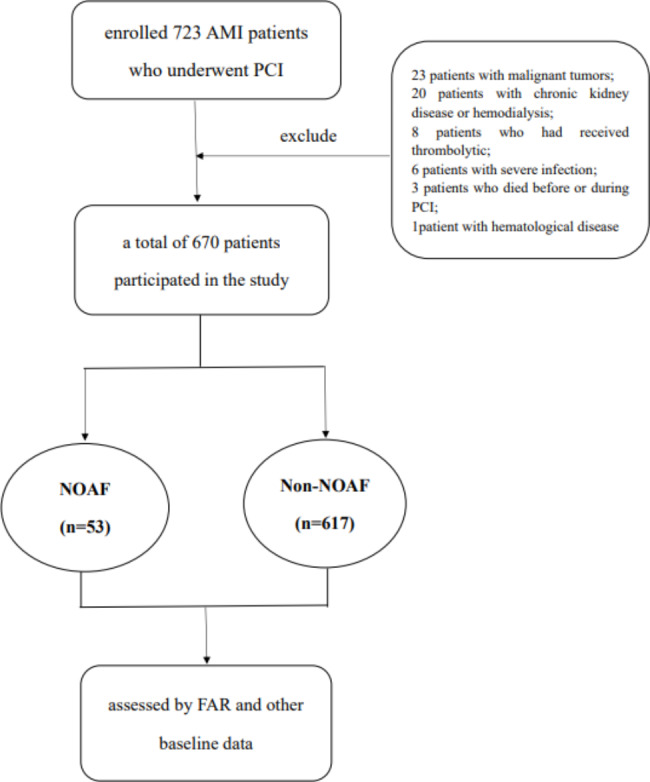
We retrospectively analyzed the incidence of NOAF during hospitalization and follow-up in 670 patients with AMI after PCI. Data were collected on patient age, sex, body mass index, medical history, current medication, heart failure, laboratory tests, culprit blood vessels, echocardiographic characteristics, and AMI type. The enrolled patients were divided into NOAF and non-NOAF groups. The baseline characteristics of patients in the two groups were compared, and the predictive correlation between FAR and NOAF was evaluated using logistic regression analysis and the receiver operating characteristic curve.
Fifty-three (7.9%) patients developed NOAF during hospitalization. The occurrence of NOAF was found to be independently associated with higher FAR besides older age, higher neutrophil count, greater left atrial size, worse Killip class upon admission, lower body mass index, lower platelet count, lower left ventricle ejection fraction, and target left circumflex artery disease. FAR exhibited a better predictive value for the occurrence of NOAF during hospitalization (area under the curve, 0.732; 95% confidence interval, 0.659-0.808).
FAR is a robust tool for predicting NOAF risk during hospitalization in patients with AMI after PCI and has a better predictive value than serum fibrin and serum albumin levels alone.
新发心房颤动(NOAF)是急性心肌梗死(AMI)患者经皮冠状动脉介入治疗(PCI)的常见不良后果,与住院时间和预后密切相关。近年来,血清纤维蛋白原与白蛋白比值(FAR)作为一种新的炎症和血栓形成标志物,已被用于预测冠状动脉疾病的严重程度和预后。我们的研究旨在探讨 AMI 患者 PCI 后住院期间 FAR 与 NOAF 之间的关系。
我们回顾性分析了 670 例 AMI 患者 PCI 后住院及随访期间的 NOAF 发生率。收集患者年龄、性别、体重指数、既往病史、当前用药、心力衰竭、实验室检查、罪犯血管、超声心动图特征和 AMI 类型等数据。将纳入的患者分为 NOAF 和非 NOAF 组。比较两组患者的基线特征,并通过逻辑回归分析和受试者工作特征曲线评估 FAR 与 NOAF 的预测相关性。
53 例(7.9%)患者在住院期间发生 NOAF。NOAF 的发生与 FAR 升高有关,而与年龄较大、中性粒细胞计数较高、左心房较大、入院时 Killip 分级较差、体重指数较低、血小板计数较低、左心室射血分数较低以及目标回旋支病变有关。FAR 对住院期间 NOAF 的发生具有更好的预测价值(曲线下面积,0.732;95%置信区间,0.659-0.808)。
FAR 是预测 AMI 患者 PCI 后住院期间 NOAF 风险的有效工具,其预测价值优于血清纤维蛋白和血清白蛋白水平。