Solomon Benjamin D, Khatri Purvesh
Department of Pediatrics, Division of Allergy and Immunology, Stanford University, Palo Alto, Calif.
Institute for Immunity, Transplantation, and Infection, School of Medicine, Stanford University, Palo Alto, Calif; Department of Medicine, Center for Biomedical Informatics Research, School of Medicine, Stanford University, Palo Alto, Calif.
J Allergy Clin Immunol. 2025 Jan;155(1):213-218.e4. doi: 10.1016/j.jaci.2024.09.006. Epub 2024 Sep 13.
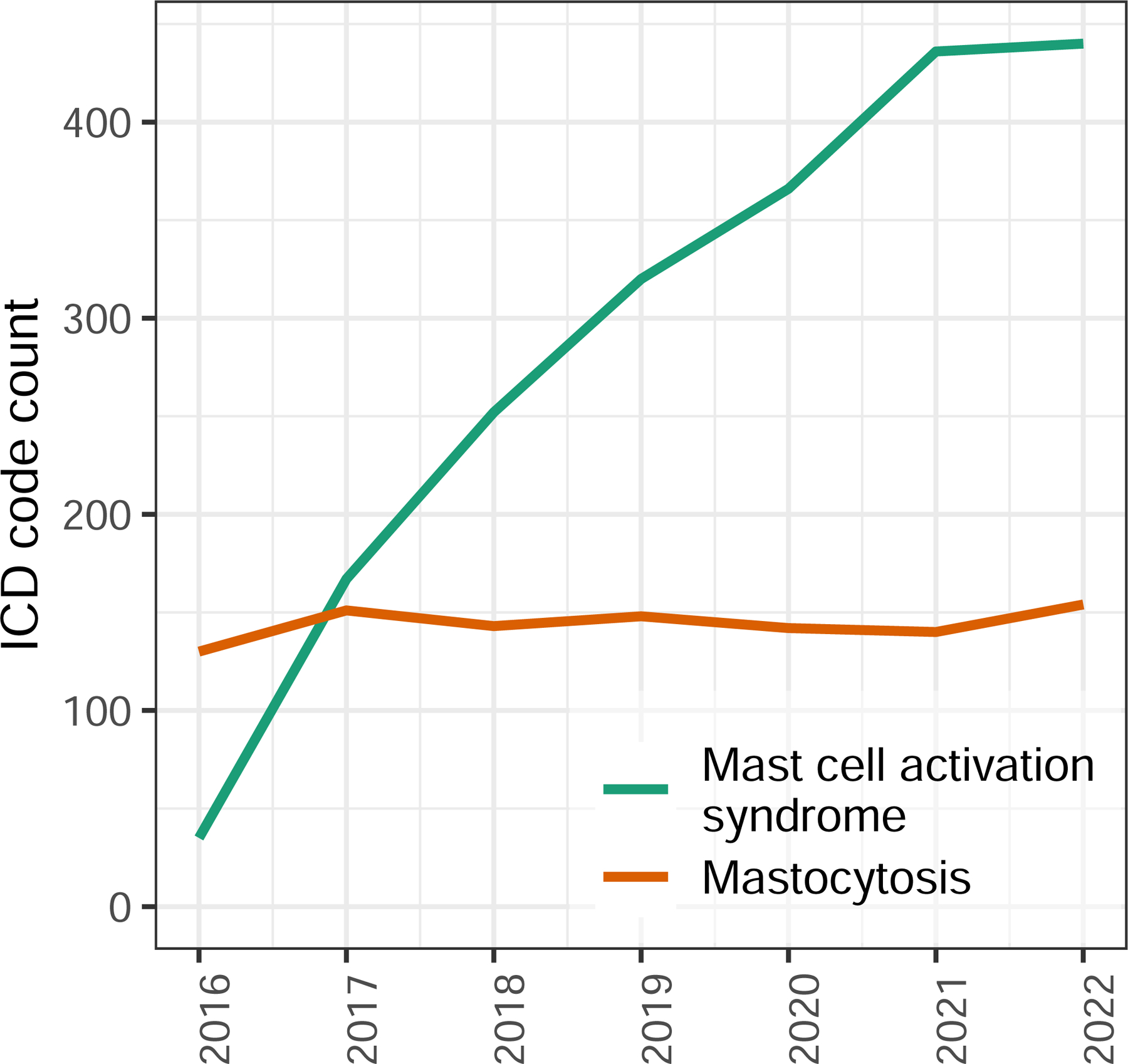
The rate of diagnosis of mast cell activation syndrome (MCAS) has increased since the disorder's original description as a mastocytosis-like phenotype. While a set of consortium MCAS criteria is well described and widely accepted, this increase occurs in the setting of a broader set of proposed alternative MCAS criteria.
Effective diagnostic criteria must minimize the range of unrelated diagnoses that can be erroneously classified as the condition of interest. We sought to determine if the symptoms associated with alternative MCAS criteria result in less concise or consistent diagnostic alternatives, reducing diagnostic specificity.
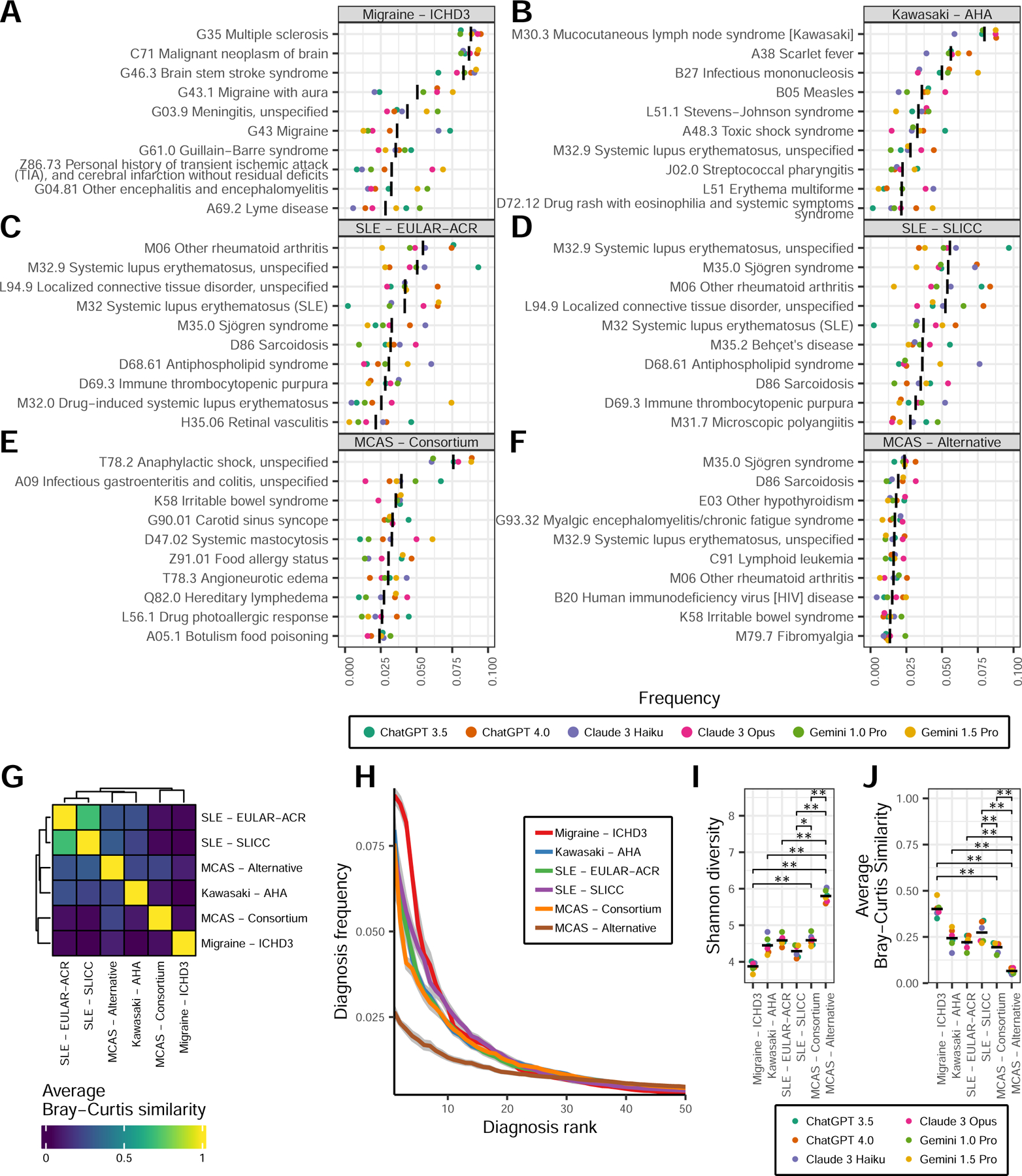
We used multiple large language models, including ChatGPT, Claude, and Gemini, to bootstrap the probabilities of diagnoses that are compatible with consortium or alternative MCAS criteria. We utilized diversity and network analyses to quantify diagnostic precision and specificity compared to control diagnostic criteria including systemic lupus erythematosus, Kawasaki disease, and migraines.
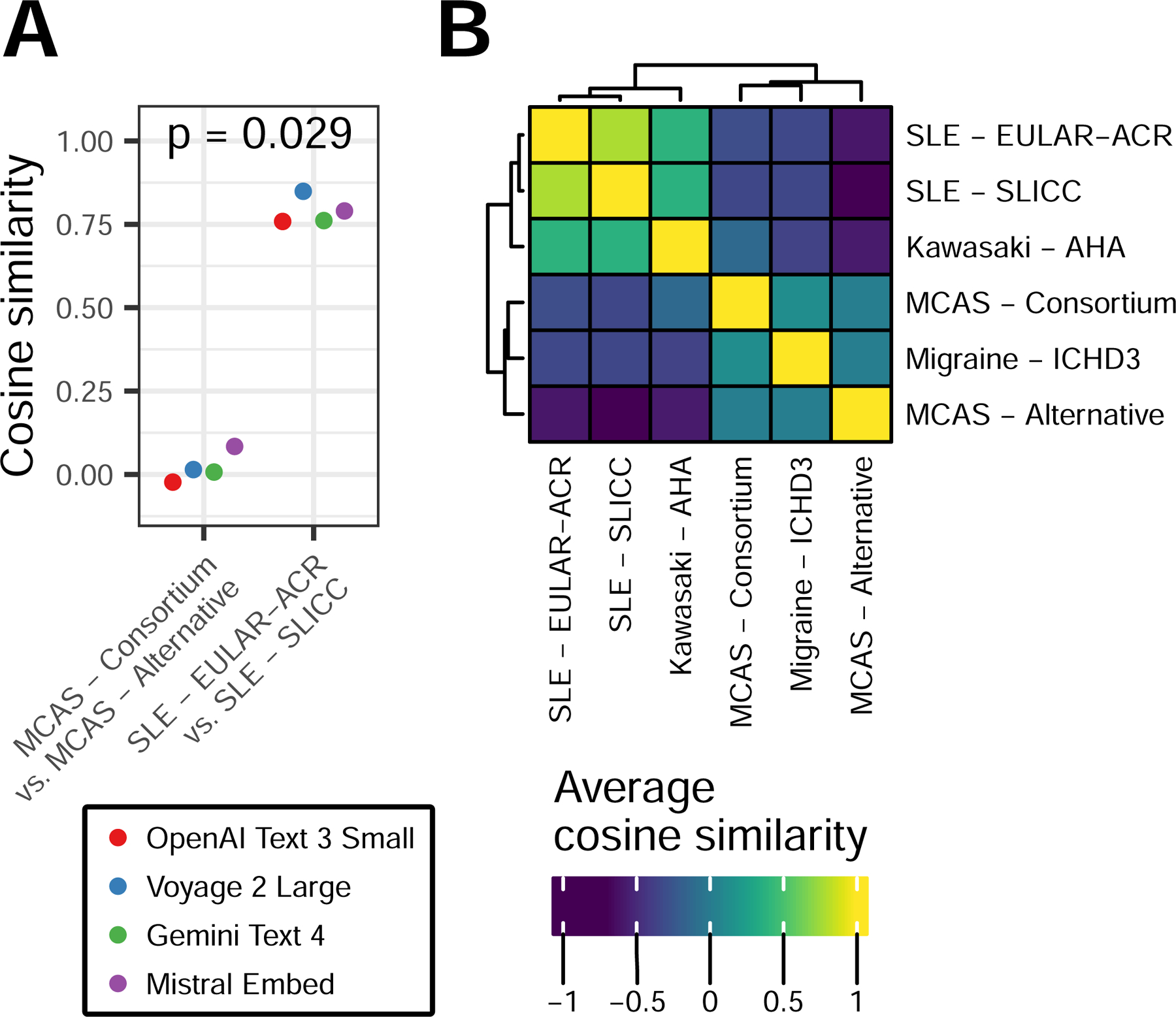
Compared to consortium MCAS criteria, alternative MCAS criteria are associated with more variable (Shannon diversity 5.8 vs 4.6, respectively; P = .004) and less precise (mean Bray-Curtis similarity 0.07 vs 0.19, respectively; P = .004) diagnoses. The diagnosis networks derived from consortium and alternative MCAS criteria had lower between-network similarity compared to the similarity between diagnosis networks derived from 2 distinct systemic lupus erythematosus criteria (cosine similarity 0.55 vs 0.86, respectively; P = .0022).
Alternative MCAS criteria are associated with a distinct set of diagnoses compared to consortium MCAS criteria and have lower diagnostic consistency. This lack of specificity is pronounced in relation to multiple control criteria, raising the concern that alternative criteria could disproportionately contribute to MCAS overdiagnosis, to the exclusion of more appropriate diagnoses.
自肥大细胞活化综合征(MCAS)最初被描述为类肥大细胞增多症表型以来,其诊断率有所上升。虽然一套联合MCAS标准已得到充分描述并被广泛接受,但这种增加是在一系列更广泛的替代性MCAS标准的背景下发生的。
有效的诊断标准必须将可能被错误分类为感兴趣疾病的无关诊断范围降至最低。我们试图确定与替代性MCAS标准相关的症状是否会导致诊断选择不那么简洁或一致,从而降低诊断特异性。
我们使用了多个大语言模型,包括ChatGPT、Claude和Gemini,来推算与联合或替代性MCAS标准相符的诊断概率。我们利用多样性和网络分析来量化与包括系统性红斑狼疮、川崎病和偏头痛在内的对照诊断标准相比的诊断精度和特异性。
与联合MCAS标准相比,替代性MCAS标准与更多变(香农多样性分别为5.8和4.6;P = 0.004)和更不精确(平均布雷-柯蒂斯相似度分别为0.07和0.19;P = 0.004)的诊断相关。与源自两种不同系统性红斑狼疮标准的诊断网络之间的相似度相比,源自联合和替代性MCAS标准的诊断网络之间的网络间相似度更低(余弦相似度分别为0.55和0.86;P = 0.0022)。
与联合MCAS标准相比,替代性MCAS标准与一组不同的诊断相关,且诊断一致性较低。这种缺乏特异性在与多个对照标准的比较中很明显,这引发了人们的担忧,即替代性标准可能会不成比例地导致MCAS过度诊断,从而排除了更合适的诊断。