Pon Avudaiappan Arjun, Prabhakar Pushan, Lusnia Ciara, Ganiyani Mohmmad Arfat, Rubens Muni, Garje Rohan, Eldefrawy Ahmed, Manoharan Murugesan
Department of Urologic Oncology Surgery, Miami Cancer Institute, Miami, Florida, USA.
Herbert Wertheim College of Medicine, Florida International University, Miami, FL, USA.
Transl Androl Urol. 2024 Aug 31;13(8):1486-1497. doi: 10.21037/tau-24-139. Epub 2024 Aug 16.
Neoadjuvant chemotherapy with radical cystectomy (RC) is the preferred first-line treatment for localized muscle-invasive bladder cancer (MIBC). Due to the concern about morbidity associated with RC, the elderly population considers bladder preservation alternatives. Guidelines suggest partial cystectomy (PC) can be considered a viable option in carefully selected individuals. We used the National Cancer Database (NCDB) to compare the overall survival (OS) among octogenarians treated with PC and RC.
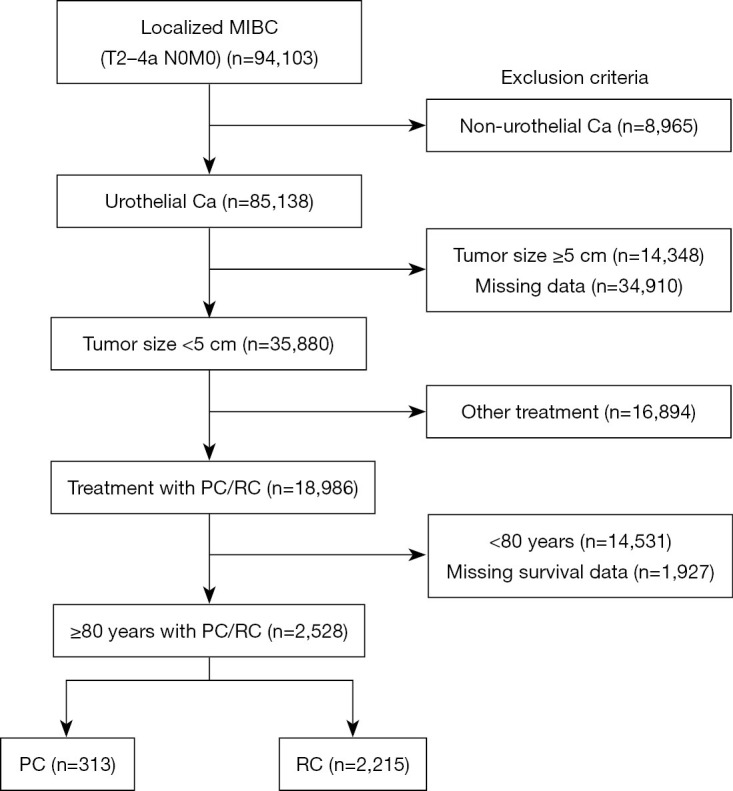
Using NCDB, we retrospectively evaluated individuals aged 80 years and above diagnosed with localized MIBC (cT2-4aN0M0) with tumor size less than 5 cm and urothelial histology between 2004 and 2018. Our primary cohort was divided into the RC cohort, which included patients who underwent RC with or without chemotherapy/radiotherapy, and the PC cohort, which included those who underwent PC. After propensity-matching, we compared the OS.
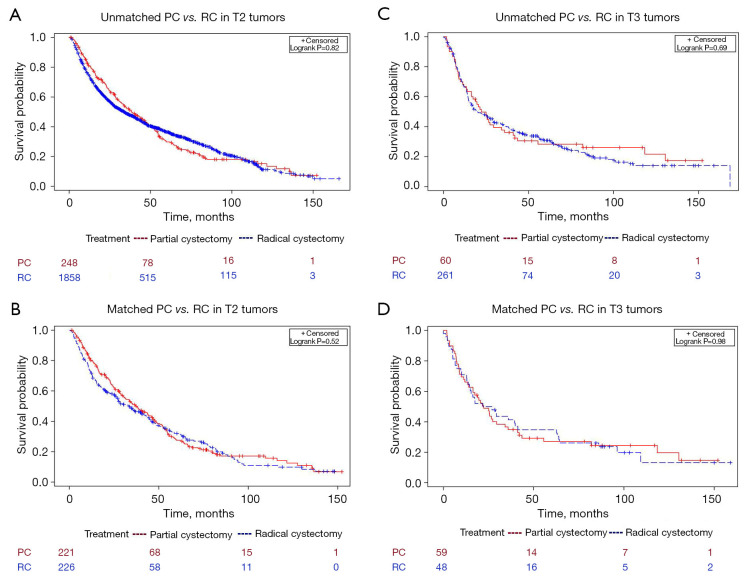
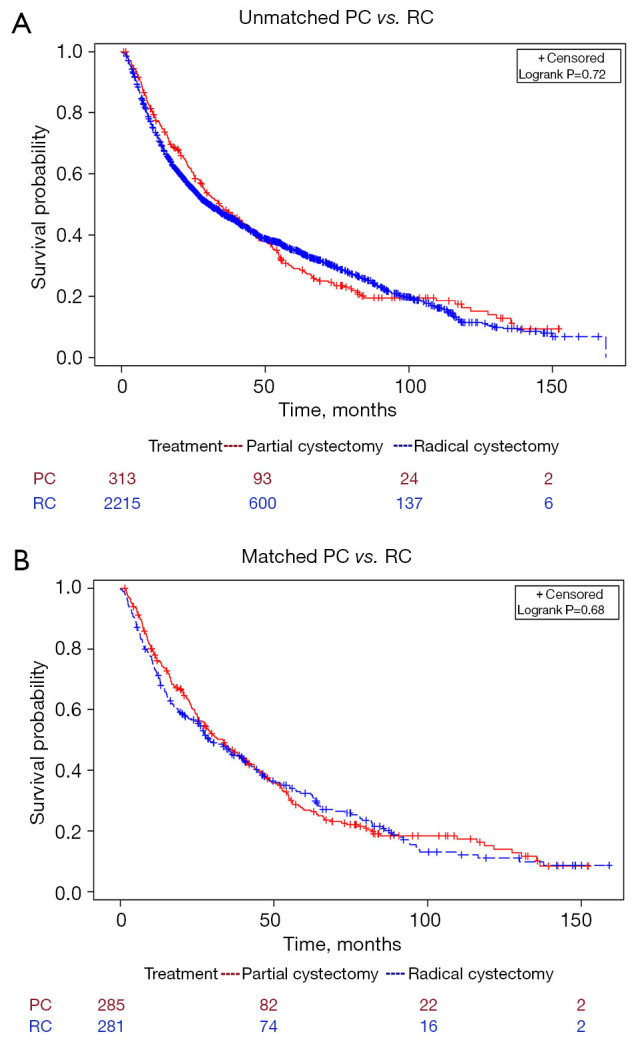
Of 94,104 patients with MIBC, 2,528 octogenarians met our selection criteria. Among them, 313 were treated with PC, and 2,215 were treated with RC. A total of 151 (48.2%) PC patients had pelvic lymph node dissection, while 1,967 (88.8%) RC patients had lymph node dissection (P<0.001). The OS for matched PC and RC was 33.4 and 29.9 months, respectively (P=0.68). In T2 tumors, the OS for PC and RC was 37 and 33.5 months, respectively (P=0.52); for T3 tumors, the OS was 22.3 and 24.4 months, respectively (P=0.98).
Our study compared PC and RC in octogenarians with localized MIBC and observed that PC is safe and not inferior to RC in carefully selected octogenarians. The role of PC needs further exploration by comparing or integrating with strategies like concurrent chemoradiation to improve the oncological and survival outcomes.
新辅助化疗联合根治性膀胱切除术(RC)是局限性肌层浸润性膀胱癌(MIBC)的首选一线治疗方法。由于担心与RC相关的发病率,老年人群考虑膀胱保留替代方案。指南建议,在经过仔细挑选的个体中,部分膀胱切除术(PC)可被视为一种可行的选择。我们使用国家癌症数据库(NCDB)比较接受PC和RC治疗的八旬老人的总生存期(OS)。
利用NCDB,我们回顾性评估了2004年至2018年间年龄在80岁及以上、诊断为局限性MIBC(cT2-4aN0M0)、肿瘤大小小于5 cm且组织学类型为尿路上皮癌的个体。我们的主要队列分为RC队列(包括接受或未接受化疗/放疗的RC患者)和PC队列(包括接受PC的患者)。在进行倾向匹配后,我们比较了OS。
在94,104例MIBC患者中,2,528例八旬老人符合我们的入选标准。其中,313例接受了PC治疗,2,215例接受了RC治疗。共有151例(48.2%)PC患者进行了盆腔淋巴结清扫,而1,967例(88.8%)RC患者进行了淋巴结清扫(P<0.001)。匹配后的PC和RC的OS分别为33.4个月和29.9个月(P=0.68)。在T2期肿瘤中,PC和RC的OS分别为37个月和33.5个月(P=0.52);在T3期肿瘤中,OS分别为22.3个月和24.4个月(P=0.98)。
我们的研究比较了八旬局限性MIBC患者的PC和RC,观察到在经过仔细挑选的八旬老人中,PC是安全的且不劣于RC。PC的作用需要通过与同步放化疗等策略进行比较或整合来进一步探索,以改善肿瘤学和生存结果。