Trung Nguyen Kien, Van Dang Ba, Thai Pham Dung, Viet Tran Tien, Dinh Le Tuan, Tien Nguyen Son, Minh Vu Duong, Tien Le Dung, Van Nguyen Bang, Anh Vu Hai, Manh Do Hung, Quang Nguyen Huy, Ba Ta Thang, Huy Duong Hoang, Pham Vu Thu Ha, Duy Nguyen Toan, Hong Le Trung, Van Ngo Dan, Dinh Hoa Trung, Luong Cong Thuc
Center of Emergency, Critical Care Medicine and Clinical Toxicology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam.
Department of Infectious Diseases, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam.
Clin Med Insights Case Rep. 2024 Sep 13;17:11795476241277663. doi: 10.1177/11795476241277663. eCollection 2024.
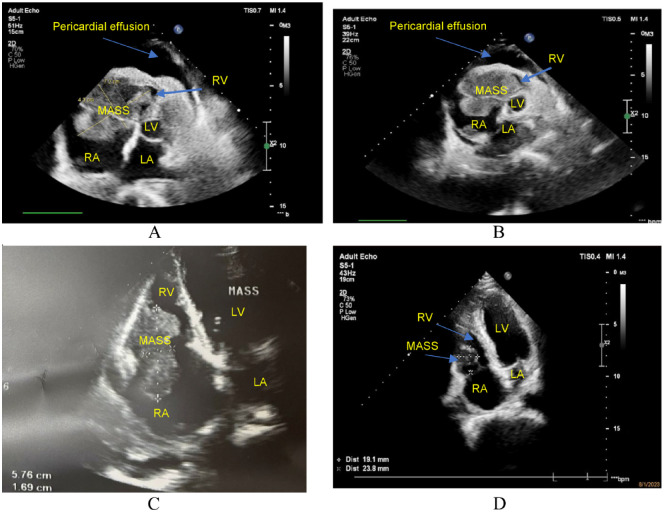
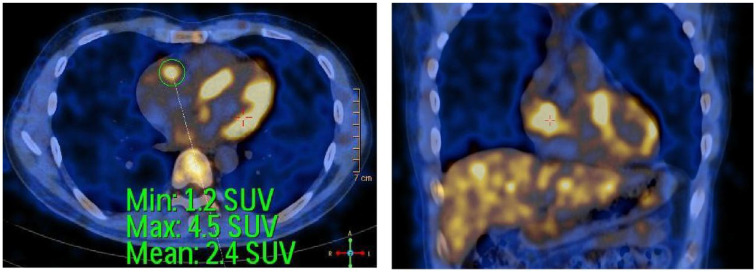
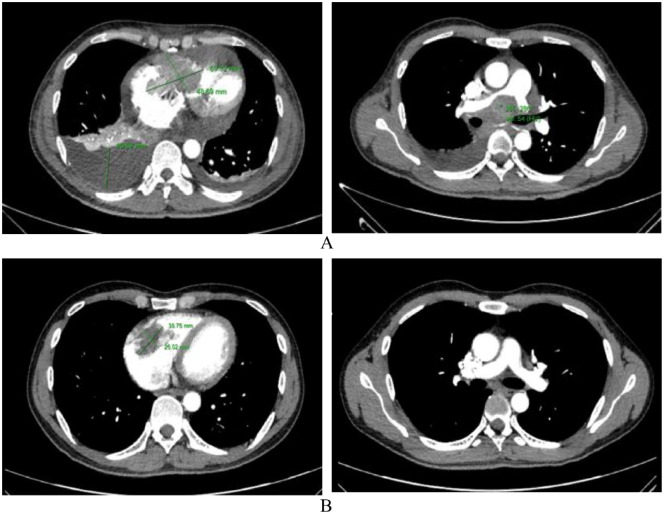
Heart tumors are sporadic. Secondary heart tumors are 30 times more common than primary ones. Depending on the location and origin of the tumor, clinical pictures vary from asymptomatic to severe manifestations such as arrhythmia, heart failure, pericardial effusion, and cardiogenic shock. We report hereby a rare case who presented with faint clinical symptoms, rapidly progressing to right heart failure within a month. Echocardiography and computed tomography of the chest revealed a tumor in the right heart chamber of 72.0 × 43.0 mm, in addition to large mediastinal lymph and left supraclavicular lymph nodes, cardiogenic shock appeared 4 days after admission. Through examination, it was suspected that this was a cardiac lymphoma. The patient was treated with 2 mg methylprednisolone per kg body weight. Symptoms of cardiogenic shock improved significantly and disappeared after 6 hours of treatment. After supraclavicular lymph node biopsy and immunohistochemistry, the final result was diagnosed as diffuse large B-cell non-Hodgkin lymphoma with large lymphoma in the right heart. The patient received chemotherapy with the R-CHOP regimen (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisolone). Re-examination before the 5th chemotherapy cycle showed no signs of right heart failure, normal self-activity, and no dyspnea on exertion, and the tumor size in the heart on the echocardiogram was 23.8 × 19.1 mm. The report shows that a large right heart tumor with a clinical picture of cardiogenic shock in a patient with diffuse large B-cell non-Hodgkin's lymphoma was well-responded to initial treatment with methylprednisolone at a dose of 2 mg/kg body weight and R-CHOP chemotherapy.
心脏肿瘤较为散在。继发性心脏肿瘤比原发性心脏肿瘤常见30倍。根据肿瘤的位置和起源,临床表现从无症状到严重表现不等,如心律失常、心力衰竭、心包积液和心源性休克。我们在此报告一例罕见病例,该患者临床症状轻微,在一个月内迅速进展为右心衰竭。超声心动图和胸部计算机断层扫描显示右心室内有一个72.0×43.0mm的肿瘤,此外还有肿大的纵隔淋巴结和左锁骨上淋巴结,入院4天后出现心源性休克。经检查,怀疑这是一例心脏淋巴瘤。患者接受了每公斤体重2mg甲泼尼龙的治疗。心源性休克症状在治疗6小时后明显改善并消失。经锁骨上淋巴结活检及免疫组化检查,最终结果诊断为右心弥漫大B细胞非霍奇金淋巴瘤伴大淋巴瘤。患者接受了R-CHOP方案(利妥昔单抗、环磷酰胺、阿霉素、长春新碱和泼尼松龙)化疗。第5个化疗周期前复查显示无右心衰竭迹象,自主活动正常,活动时无呼吸困难,超声心动图显示心脏肿瘤大小为23.8×19.1mm。该报告表明,一例弥漫大B细胞非霍奇金淋巴瘤患者出现伴有心源性休克临床表现的巨大右心肿瘤,初始接受每公斤体重2mg甲泼尼龙治疗及R-CHOP化疗后反应良好。