Department of Anesthesia and Perioperative Medicine, Faculty of Medicine, Hospital Clínico de la Universidad de Chile, Universidad de Chile, Santiago, Chile.
Faculty of Medicine, Universidad de Chile, Santiago, Chile.
BMC Anesthesiol. 2024 Sep 17;24(1):329. doi: 10.1186/s12871-024-02718-z.
To examine the relationship between neutrophil-to-lymphocyte ratio (NLR), age, and mortality rates after emergency surgery.
In this observational study, a total of 851 patients undergoing emergency surgery between January 2022 and January 2023 were retrospective examined. Using 30 and 180 days mortality data, NLR differences and receiver operating characteristic (ROC) curves were analyzed using a 65-year threshold. A multiple logistic regression model was constructed incorporating age and NLR. Finally, Kaplan-Meier curves were constructed for mortality.
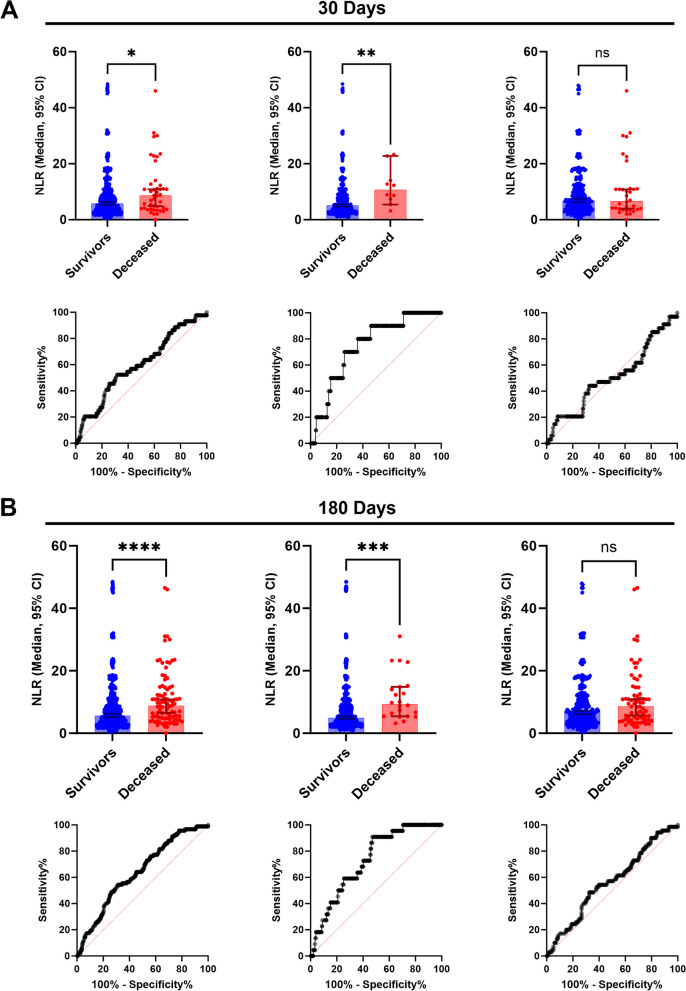
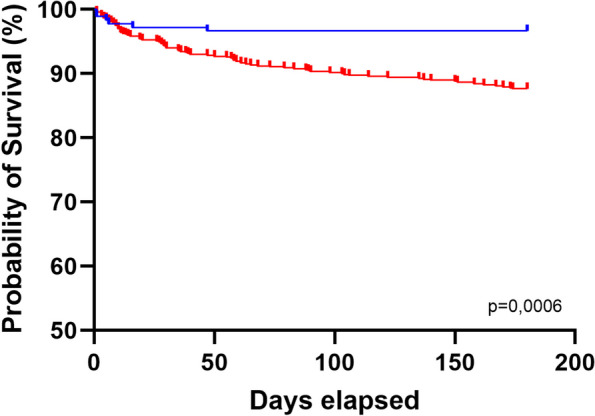
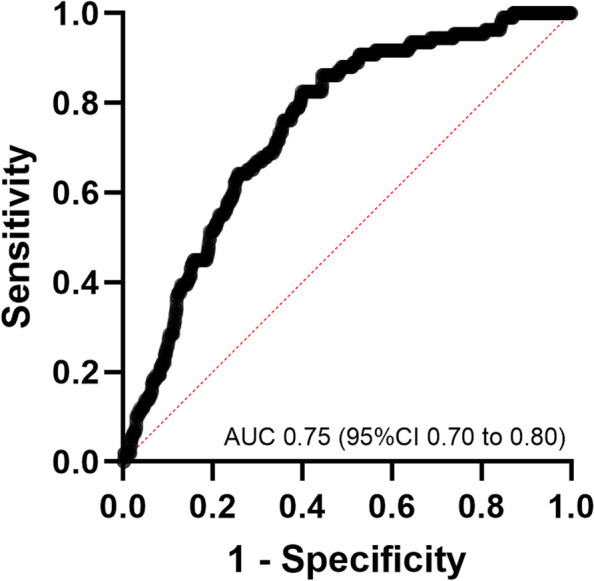
Among 851 patients, the 30 and 180 days mortality rates were 5.2% and 10.8%, respectively. Median NLR in 30 days was 5.6 (3.1 to 9.6) in survivors and 8.7 (4.6 to 13.4) in deceased patients (p < 0.0001); in 180 days, it was 5.5 (3.1 to 9.8) and 8.8 (4.8 to 14.5), respectively (p < 0.0001). In the 30- and 180-days mortality analyses, median NLRs were 5.1 (2.9 to 8.9) and 4.9 (2.9 to 8.8) in survivors and 10.6 (6.9 to 16.6) and 9.3 (5.4 to 14.9) in deceased patients aged < 65 years, respectively. The ROC AUC in patients younger than 65 years was higher for 30 days (AUC 0.75; 95% CI 0.72 to 0.87) and 180 days (AUC 0.73; 95% CI 0.64 to 0.81). Multivariate logistic regression revealed that the NLR (odds ratio, 1.03 [95% CI 1.005 to 1.053; p = 0.0133) and age (odds ratio, 1.05 [95% CI 1.034 to 1.064; p < 0.0001) significantly contributed to the model. Survival analysis revealed differences in the 180 days mortality (p = 0.0006).
We observed differences in preoperative NLR between patients who survived and those who died after emergency surgery. Age impacts the use of NLR as a mortality risk factor.
NCT06549101, retrospectively registered.
探讨中性粒细胞与淋巴细胞比值(NLR)、年龄与急诊手术后死亡率的关系。
本观察性研究回顾性分析了 2022 年 1 月至 2023 年 1 月期间接受急诊手术的 851 例患者。使用 30 天和 180 天死亡率数据,使用 65 岁阈值分析 NLR 差异和受试者工作特征(ROC)曲线。构建了包含年龄和 NLR 的多因素逻辑回归模型。最后,构建了死亡率的 Kaplan-Meier 曲线。
在 851 例患者中,30 天和 180 天的死亡率分别为 5.2%和 10.8%。存活者 30 天 NLR 中位数为 5.6(3.1 至 9.6),死亡者为 8.7(4.6 至 13.4)(p<0.0001);180 天 NLR 中位数分别为 5.5(3.1 至 9.8)和 8.8(4.8 至 14.5)(p<0.0001)。在 30 天和 180 天的死亡率分析中,存活者 NLR 中位数为 5.1(2.9 至 8.9),死亡者 NLR 中位数为 10.6(6.9 至 16.6);存活者年龄<65 岁,其 NLR 中位数为 4.9(2.9 至 8.8),死亡者 NLR 中位数为 9.3(5.4 至 14.9)。年龄<65 岁患者的 30 天(AUC 0.75;95%CI 0.72 至 0.87)和 180 天(AUC 0.73;95%CI 0.64 至 0.81)ROC 曲线 AUC 更高。多变量逻辑回归显示 NLR(比值比,1.03[95%CI 1.005 至 1.053;p=0.0133])和年龄(比值比,1.05[95%CI 1.034 至 1.064;p<0.0001)对模型有显著贡献。生存分析显示,180 天死亡率存在差异(p=0.0006)。
我们观察到急诊手术后存活患者与死亡患者术前 NLR 存在差异。年龄影响 NLR 作为死亡率风险因素的应用。
NCT06549101,回顾性注册。