Jin Haijiao, Fang Wei, Wang Ling, Zang Xiujuan, Deng Yueyi, Wu Guoqing, Li Ying, Chen Xiaonong, Wang Niansong, Jiang Gengru, Guo Zhiyong, Wang Xiaoxia, Qi Yinghui, Lv Shifan, Ni Zhaohui
Department of Nephrology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Molecular Cell Laboratory for Kidney Disease, Shanghai, China.
Kidney Int Rep. 2024 Jun 27;9(9):2627-2634. doi: 10.1016/j.ekir.2024.06.032. eCollection 2024 Sep.
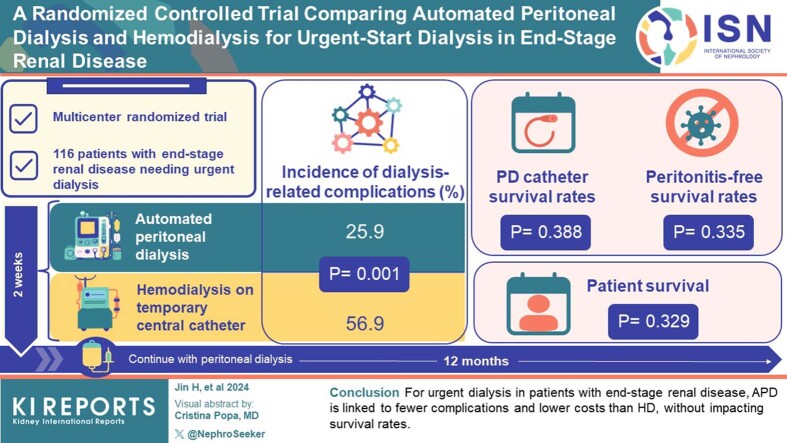
Peritoneal dialysis (PD) shows promise for urgent-start dialysis in end-stage renal disease (ESRD), with automated PD (APD) having advantages. However, there is limited multicenter randomized controlled trial (RCT) evidence comparing APD with temporary hemodialysis (HD) for this indication in China.
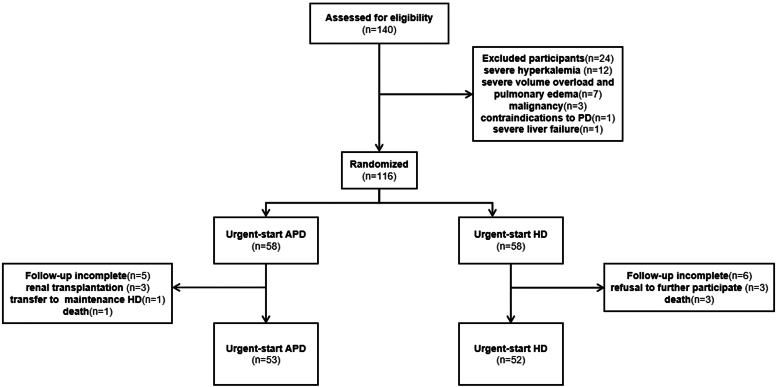
This multicenter RCT enrolled 116 patients with ESRD requiring urgent dialysis from 11 hospitals, randomized to APD or HD. Patients underwent a 2-week treatment with APD or HD via a temporary central venous catheter (CVC), followed by a maintenance PD. Outcomes were assessed over 12 months during 8 visits. The primary outcome was dialysis-related complications.
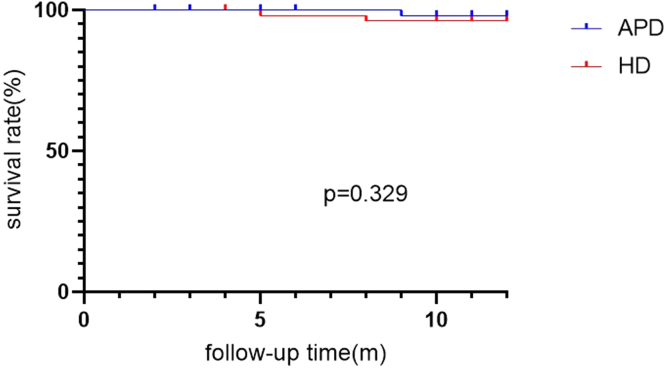
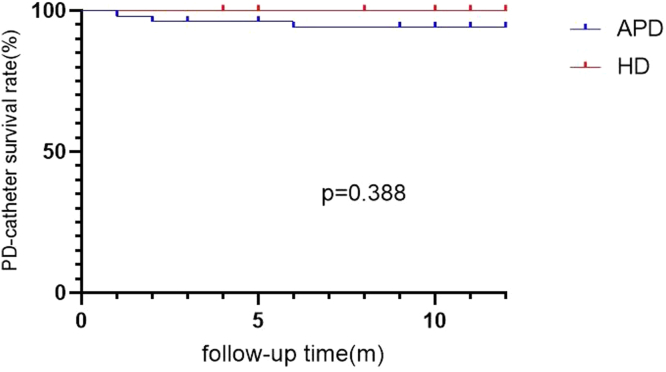
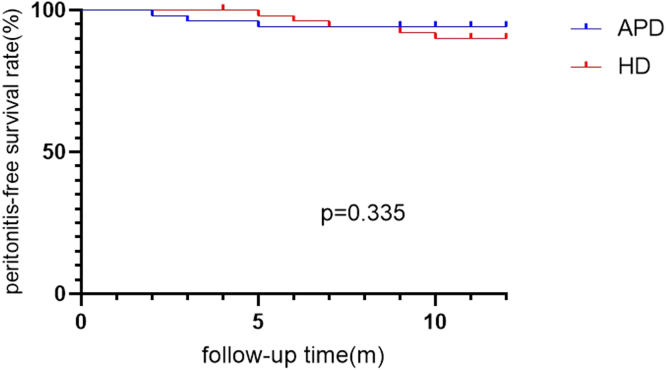
The 1-year incidence of dialysis-related complications was significantly lower in the APD group than in the HD group (25.9% vs. 56.9%, = 0.001). No significant differences were found between the groups in terms of PD catheter survival rates ( = 0.388), peritonitis-free survival rates ( = 0.335), and patient survival rates ( = 0.329). In terms of health economics, the total direct medical cost of the initial hospitalization for patients with ESRD was significantly lower in the APD group (27,008.39 CNY) than in the HD group (42,597.54 CNY) ( = 0.001), whereas the duration of the first hospital stay showed no significant difference ( = 0.424).
For patients with ESRD needing urgent initiation of dialysis, APD was associated with a lower incidence of dialysis-related complications and lower initial hospitalization costs compared with HD, with no significant differences in PD catheter survival rate, peritonitis-free survival rates, or patient survival rates. These findings can guide clinical decision-making for the optimal dialysis modality for patients requiring urgent dialysis initiation.
腹膜透析(PD)在终末期肾病(ESRD)的紧急起始透析方面显示出前景,自动化腹膜透析(APD)具有优势。然而,在中国,针对该适应症比较APD与临时血液透析(HD)的多中心随机对照试验(RCT)证据有限。
这项多中心RCT纳入了来自11家医院的116例需要紧急透析的ESRD患者,随机分为APD组或HD组。患者通过临时中心静脉导管(CVC)接受为期2周的APD或HD治疗,随后进行维持性腹膜透析。在8次访视期间对12个月的结局进行评估。主要结局是透析相关并发症。
APD组透析相关并发症的1年发生率显著低于HD组(25.9%对56.9%,P = 0.001)。两组在腹膜透析导管生存率(P = 0.388)、无腹膜炎生存率(P = 0.335)和患者生存率(P = 0.329)方面未发现显著差异。在卫生经济学方面,ESRD患者首次住院的总直接医疗费用APD组(27,008.39元)显著低于HD组(42,597.54元)(P = 0.001),而首次住院时间无显著差异(P = 0.424)。
对于需要紧急开始透析的ESRD患者,与HD相比,APD与透析相关并发症的发生率较低以及首次住院费用较低相关,在腹膜透析导管生存率、无腹膜炎生存率或患者生存率方面无显著差异。这些发现可为需要紧急开始透析的患者选择最佳透析方式提供临床决策指导。