Parapiboon Watanyu, Sangsuk Juthamash, Nopsopon Tanawin, Pitsawong Wannapat, Tatiyanupanwong Sajja, Kanjanabuch Talerngsak, Johnson David W
Nephrology Unit, Department of Medicine, Maharat Nakhonratchasima Hospital, Nakhonratchasima, Thailand.
Department of Preventive and Social Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Kidney Int Rep. 2022 Jun 11;7(8):1866-1877. doi: 10.1016/j.ekir.2022.05.032. eCollection 2022 Aug.
We sought to evaluate the efficacy and complications of urgent-start peritoneal dialysis (PD) compared with urgent-start temporary hemodialysis (HD) followed by subsequent elective transfer to PD.
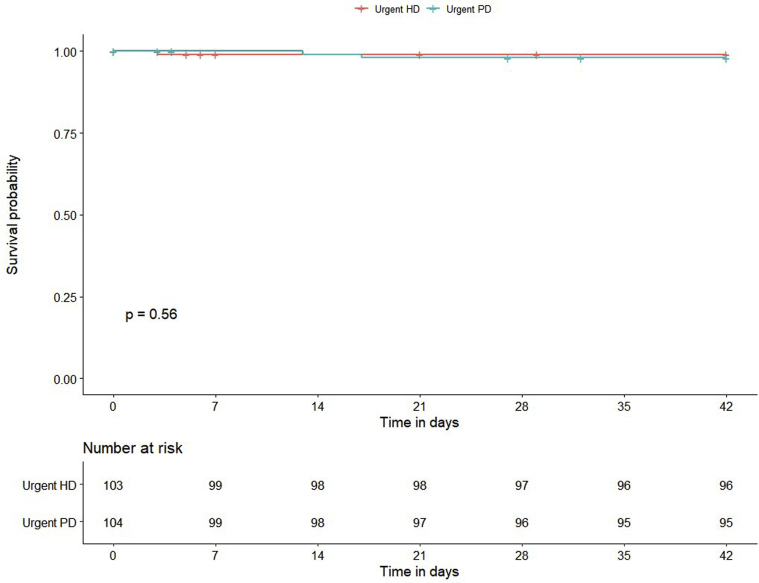
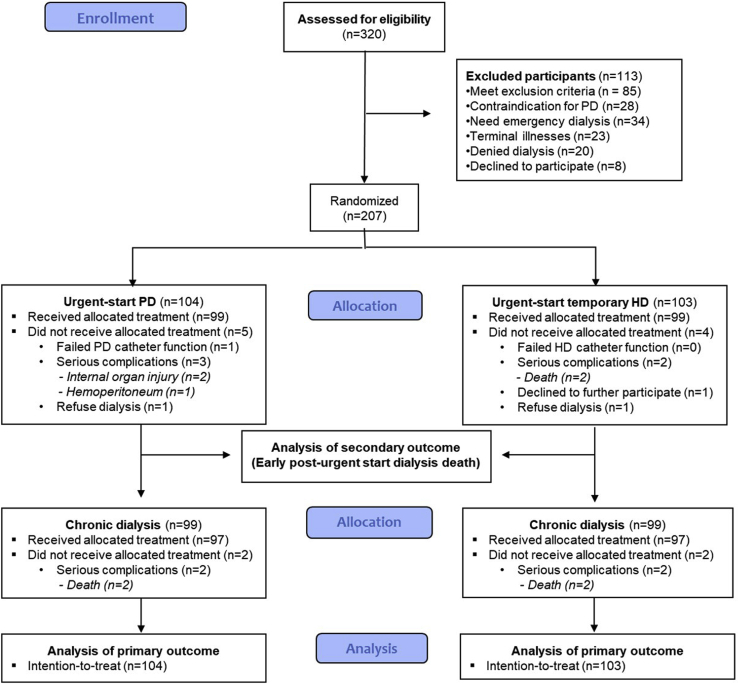
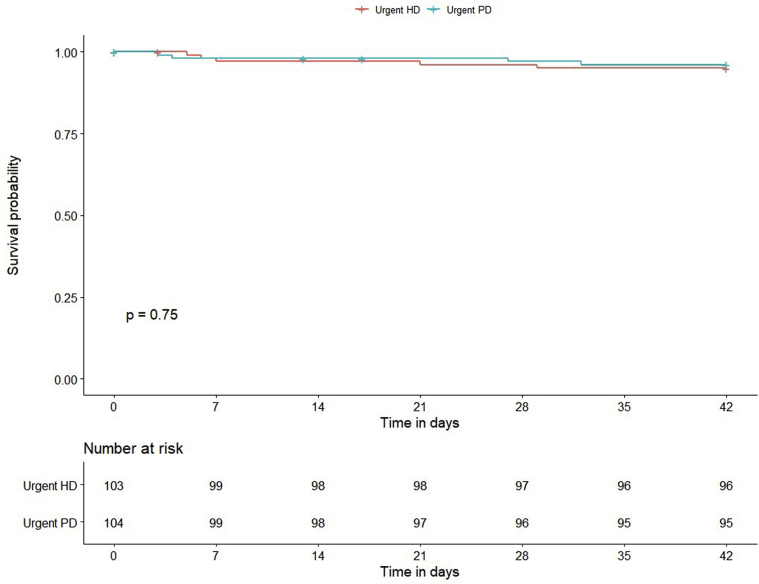
In this multicenter open-label prospective randomized controlled trial, adults with kidney failure who required immediate dialysis but did not have access to definitive dialysis were randomized to receive either urgent-start PD or urgent-start temporary HD over 2 weeks to 4 weeks followed by a transition to a chronic PD program according to the country policy. The primary outcome was the composite end point of operation-related, catheter-related, and dialysis-related complications at 6 weeks. Secondary outcomes were 6-week mortality, 6-week technique survival, and 1-week composite complications.
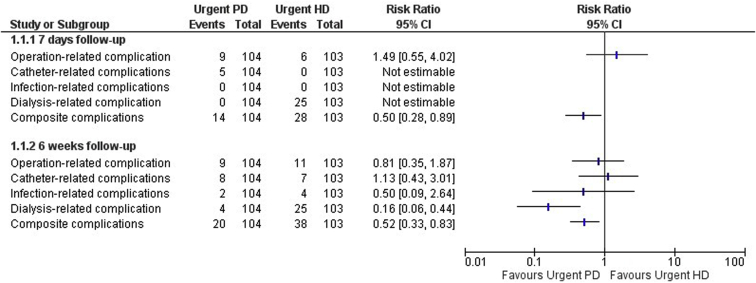
A total of 207 participants requiring urgent-start dialysis were enrolled from 3 tertiary hospitals between November 2018 and February 2020 as follows: 104 were assigned to receive urgent-start PD, and 103 were assigned to urgent-start temporary HD. Compared with urgent-start temporary HD, urgent-start PD had a lower composite complication rate at 6 weeks (19% vs. 37%, risk ratio [RR] 0.52, 95% CI 0.33-0.83), which was primarily accounted for by a reduction in dialysis-related complications (4% vs. 24%, RR 0.16, 95% CI 0.06-0.44). No significant differences were observed between the 2 groups with respect to patient and technique survival rates at 1 week and 6 weeks.
An urgent-start PD strategy during the transition of kidney failure to chronic dialysis is safe and has fewer complications commensurate with their reduced exposure to procedural risk than urgent-start temporary HD up to 6 weeks after dialysis commencement.
我们旨在评估紧急启动腹膜透析(PD)与紧急启动临时血液透析(HD)并随后择期转为PD的疗效及并发症。
在这项多中心开放标签前瞻性随机对照试验中,将需要立即透析但无法进行确定性透析的成年肾衰竭患者随机分为两组,一组接受紧急启动的PD,另一组接受紧急启动的临时HD,为期2至4周,之后根据国家政策转为慢性PD方案。主要结局是6周时手术相关、导管相关和透析相关并发症的复合终点。次要结局包括6周死亡率、6周技术生存率和1周复合并发症。
2018年11月至2020年2月期间,从3家三级医院招募了总共207名需要紧急启动透析的参与者,具体如下:104名被分配接受紧急启动的PD,103名被分配接受紧急启动的临时HD。与紧急启动的临时HD相比,紧急启动的PD在6周时的复合并发症发生率较低(19%对37%,风险比[RR]0.52,95%置信区间0.33 - 0.83),这主要是由于透析相关并发症的减少(4%对24%,RR 0.16,95%置信区间0.06 - 0.44)。两组在1周和6周时的患者生存率和技术生存率方面未观察到显著差异。
在肾衰竭向慢性透析过渡期间,紧急启动PD策略是安全的,与紧急启动的临时HD相比,在透析开始后长达6周的时间里,其并发症更少,这与其较低的操作风险暴露程度相符。