Thumfart Julia, Wagner Steffen, Kirchner Marietta, Azukaitis Karolis, Bayazit Aysun K, Obrycki Lukasz, Canpolat Nur, Bulut Ipek Kaplan, Duzova Ali, Anarat Ali, Bessenay Lucie, Shroff Rukshana, Paripovic Dusan, Sever Lale, Candan Cengiz, Lugani Francesca, Yilmaz Alev, Yalcinkaya Fatos, Arbeiter Klaus, Kiyak Aysel, Zurowska Aleksandra, Galiano Matthias, Querfeld Uwe, Melk Anette, Schaefer Franz
Department of Pediatric Gastroenterology, Nephrology and Metabolic Diseases, Charité Universitätsmedizin, Berlin, Germany.
BHT Berliner Hochschule für Technik, Berlin, Germany.
Kidney Int Rep. 2024 Jun 12;9(9):2750-2758. doi: 10.1016/j.ekir.2024.06.009. eCollection 2024 Sep.
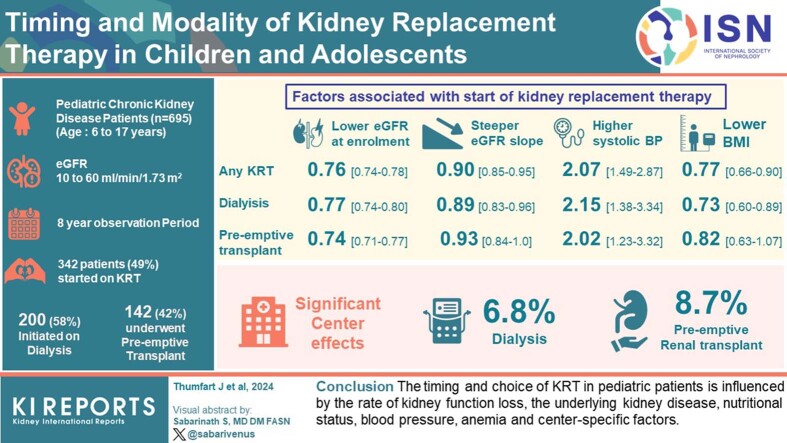
The choice and timing of kidney replacement therapy (KRT) is influenced by clinical factors, laboratory features, feasibility issues, family preferences, and clinicians' attitudes. We analyzed the factors associated with KRT modality and timing in a multicenter, multinational prospective pediatric cohort study.
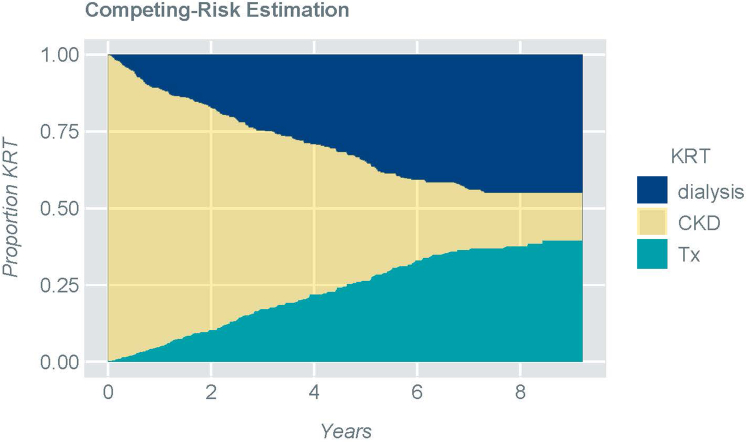
A total of 695 pediatric patients with chronic kidney disease (CKD) enrolled into the Cardiovascular Comorbidity in Children with CKD (4C) study at age 6 to 17 years with estimated glomerular filtration rate (eGFR) of 10 to 60 ml/min per 1.73 m were investigated. Competing risk regression was performed to identify factors associated with initiation of dialysis or preemptive transplantation (Tx), including primary renal diagnosis, demographics, anthropometrics, and laboratory parameters.
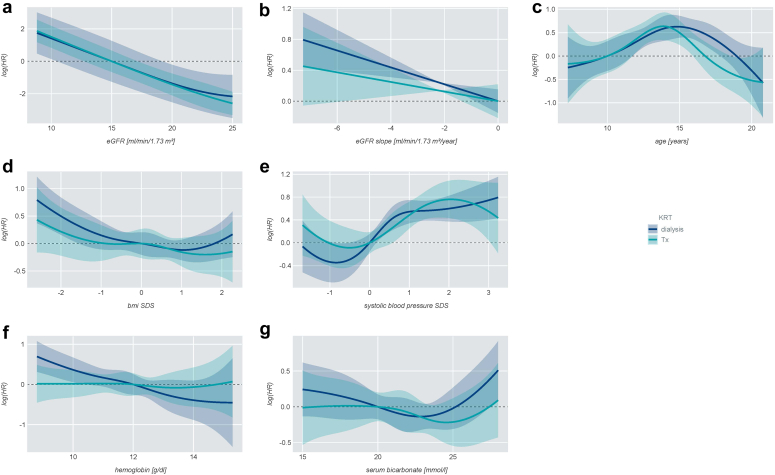
During the 8-year observation period, 342 patients (49%) started KRT. Of these, 200 patients started dialysis, whereas 142 patients underwent preemptive Tx. A lower eGFR at enrolment (Hazard ratio [HR]: 0.76 [95% confidence interval: 0.74-0.78]), a steeper eGFR slope (HR: 0.90 [0.85-0.95], and a higher systolic blood pressure SD score (SDS) (HR: 2.07 [1.49-2.87]) increased the likelihood of KRT initiation. Patients with glomerulopathies were more likely to start dialysis than children with congenital anomalies of the kidneys and urinary tracts (CAKUT) (HR: 3.81 [2.52-5.76]). Lower body mass index (BMI) SDS (HR: 0.73 [0.6-0.89]) and lower hemoglobin (HR: 0.8 [0.72-0.9]) were associated with higher likelihood of dialysis. A significant center effect was observed, accounting for 6.8% (dialysis) to 8.7% (preemptive Tx) of explained variation.
The timing and choice of KRT in pediatric patients is influenced by the rate of kidney function loss, the underlying kidney disease, nutritional status, blood pressure, anemia and center-specific factors.
肾脏替代治疗(KRT)的选择和时机受临床因素、实验室指标、可行性问题、家庭偏好及临床医生态度的影响。我们在一项多中心、跨国前瞻性儿科队列研究中分析了与KRT方式和时机相关的因素。
共有695例年龄在6至17岁、估计肾小球滤过率(eGFR)为每1.73平方米10至60毫升/分钟的慢性肾脏病(CKD)儿科患者纳入儿童CKD心血管合并症(4C)研究。采用竞争风险回归分析确定与开始透析或抢先移植(Tx)相关的因素,包括原发性肾脏诊断、人口统计学、人体测量学和实验室参数。
在8年观察期内,342例患者(49%)开始KRT。其中,200例患者开始透析,142例患者接受抢先Tx。入组时较低的eGFR(风险比[HR]:0.76[95%置信区间:0.74 - 0.78])、较陡的eGFR斜率(HR:0.90[0.85 - 0.95])以及较高的收缩压标准差评分(SDS)(HR:2.07[1.49 - 2.87])增加了开始KRT的可能性。肾小球病患者比先天性肾脏和尿路异常(CAKUT)患儿更有可能开始透析(HR:3.81[2.52 - 5.76])。较低的体重指数(BMI)SDS(HR:0.73[0.6 - 0.89])和较低的血红蛋白(HR:0.8[0.72 - 0.9])与更高的透析可能性相关。观察到显著的中心效应,占解释变异的6.8%(透析)至8.7%(抢先Tx)。
儿科患者KRT的时机和选择受肾功能丧失率、潜在肾脏疾病、营养状况、血压、贫血及中心特异性因素影响。