Department of Critical Care Medicine, the Second Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China.
Key Laboratory of Surgical Critical Care and Life Support, Xi'an Jiaotong University, Ministry of Education, Xi'an, China.
BMC Neurol. 2024 Sep 18;24(1):351. doi: 10.1186/s12883-024-03763-4.
Base excess (BE) is associated with mortality from many diseases. However, the relationship between BE and mortality in patients with ischemic stroke remains uncertain. Our aim is to investigate the relationship between BE values upon admission to the ICU and mortality rates in critically ill stroke patients.
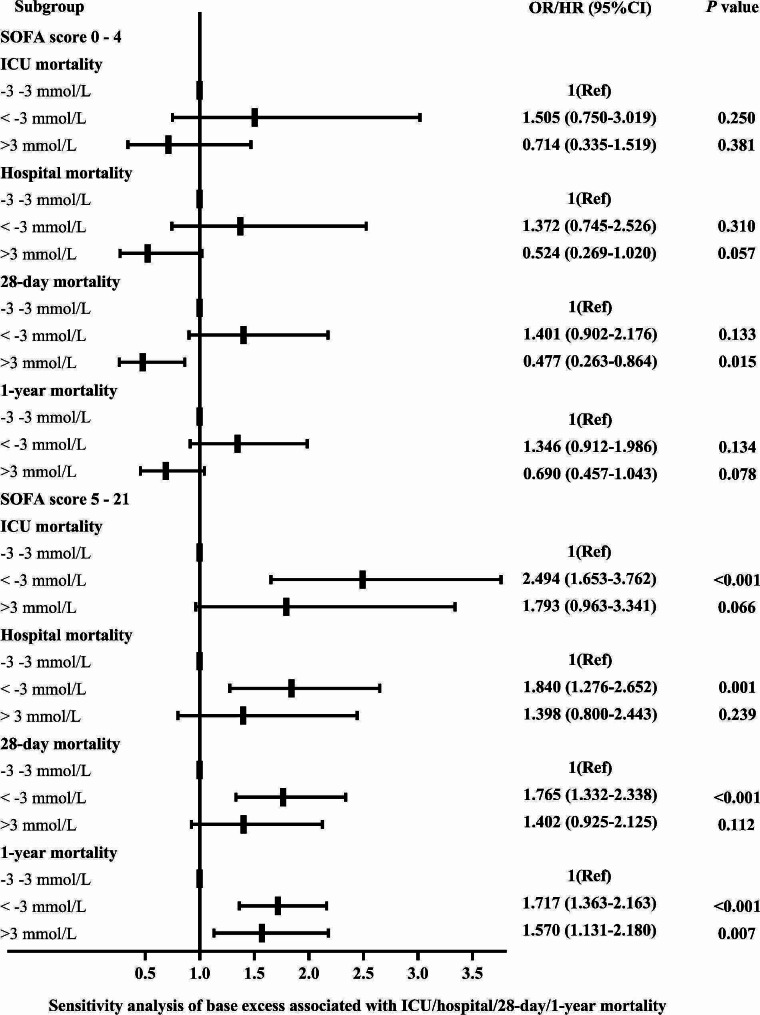
The current study enrolled 1,572 patients with ischemic stroke (863 males and 709 females). The associations of BE with intensive care unit (ICU), hospital, 28-day, and 1-year mortalities were assessed using multivariable logistic regression or Cox proportional hazards model. The potential impact of the Sequential Organ Failure Assessment (SOFA) score (< 5 or ≥ 5) on the prognostic value of BE was further evaluated with interaction and subgroup analyses.
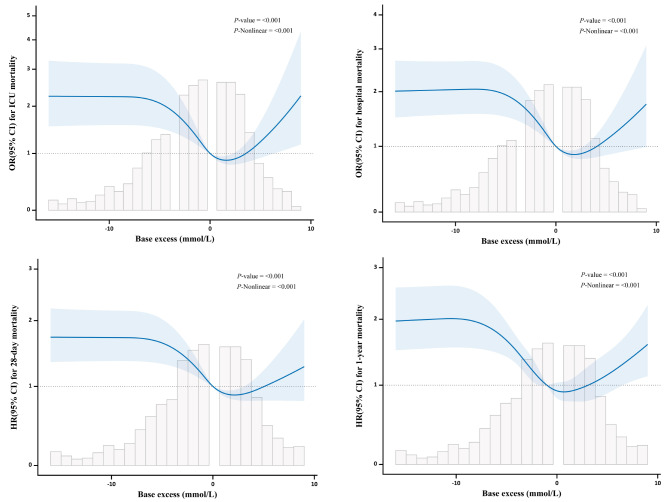
BE values less than - 3 mmol/L, greater than 3 mmol/L, and within - 3 to 3 mmol/L (normal BE) were observed in 316 (20.1%), 175 (11.1%), and 1,081 (68.8%) patients, respectively. The restricted cubic splines analyses revealed that a U-shaped curve between BE and the mortality risk. Multivariable analysis indicated that patients with low BE (<-3 mmol/L) had higher rates of ICU mortality (odds ratio [OR], 1.829; 95% confidence interval [CI], 1.281-2.612; P = 0.001), hospital mortality (OR, 1.484; 95% CI, 1.077-2.045; P = 0.016), 28-day mortality (hazard ratio [HR], 1.522; 95% CI, 1.200-1.929; P = 0.001), and 1-year mortality (HR, 1.399; 95% CI, 1.148-1.705; P = 0.001) than patients with normal BE. Subgroup analyses showed consistent results pertaining to SOFA scores ≥ 5.
In critically ill patients with ischemic stroke, an initial BE of <-3 mmol/L at ICU admission may indicate an increased risk of ICU, hospital, 28-day, and 1-year mortalities.
基础代谢过剩(BE)与许多疾病的死亡率有关。然而,BE 与缺血性脑卒中患者死亡率之间的关系尚不确定。我们的目的是探讨重症监护病房(ICU)入院时 BE 值与危重症脑卒中患者死亡率之间的关系。
本研究纳入了 1572 例缺血性脑卒中患者(男性 863 例,女性 709 例)。使用多变量逻辑回归或 Cox 比例风险模型评估 BE 与 ICU、医院、28 天和 1 年死亡率之间的关系。通过交互作用和亚组分析进一步评估序贯器官衰竭评估(SOFA)评分(<5 或≥5)对 BE 预后价值的潜在影响。
316 例(20.1%)、175 例(11.1%)和 1081 例(68.8%)患者的 BE 值分别小于-3mmol/L、大于 3mmol/L 和在-3 至 3mmol/L(正常 BE)范围内。限制性立方样条分析显示,BE 与死亡率风险之间呈 U 型曲线关系。多变量分析表明,低 BE(< -3mmol/L)患者 ICU 死亡率(优势比[OR],1.829;95%置信区间[CI],1.281-2.612;P=0.001)、医院死亡率(OR,1.484;95%CI,1.077-2.045;P=0.016)、28 天死亡率(风险比[HR],1.522;95%CI,1.200-1.929;P=0.001)和 1 年死亡率(HR,1.399;95%CI,1.148-1.705;P=0.001)均高于正常 BE 患者。亚组分析显示 SOFA 评分≥5 时结果一致。
在重症缺血性脑卒中患者中,ICU 入院时初始 BE 值<-3mmol/L 可能预示着 ICU、医院、28 天和 1 年死亡率增加的风险。