Jagt Thyrza Z, Janssen Tomas M, Sonke Jan-Jakob
Department of Radiation Oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands.
Phys Imaging Radiat Oncol. 2024 Sep 5;32:100636. doi: 10.1016/j.phro.2024.100636. eCollection 2024 Oct.
Monte Carlo (MC) based dose calculations are widely used in radiotherapy with a low statistical uncertainty, being accurate but slow. Increasing the uncertainty accelerates the calculation, but reduces quality. In online adaptive planning, however, dose is recalculated every treatment fraction, potentially decreasing the cumulative calculation error. This study aimed to evaluate the effect of higher MC statistical uncertainty in the context of daily online plan adaptation.
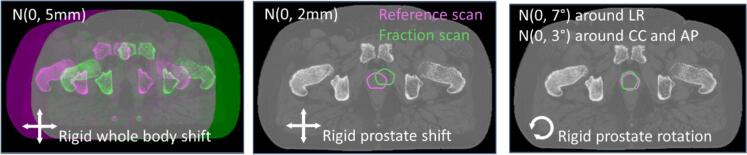
For twenty prostate cancer patients, daily plans were simulated for 5 fractions and three modes of variation: rigid whole body translations, local-rigid prostate translations and local-rigid prostate rotations. For each mode and fraction, adaptive plans were generated from a clinical reference plan using three MC uncertainty values: 1 % (standard), 2 % and 3 % per plan. Dose-volume criteria were evaluated for accumulated doses, checking plan acceptability and comparing higher uncertainty plans to the standard.
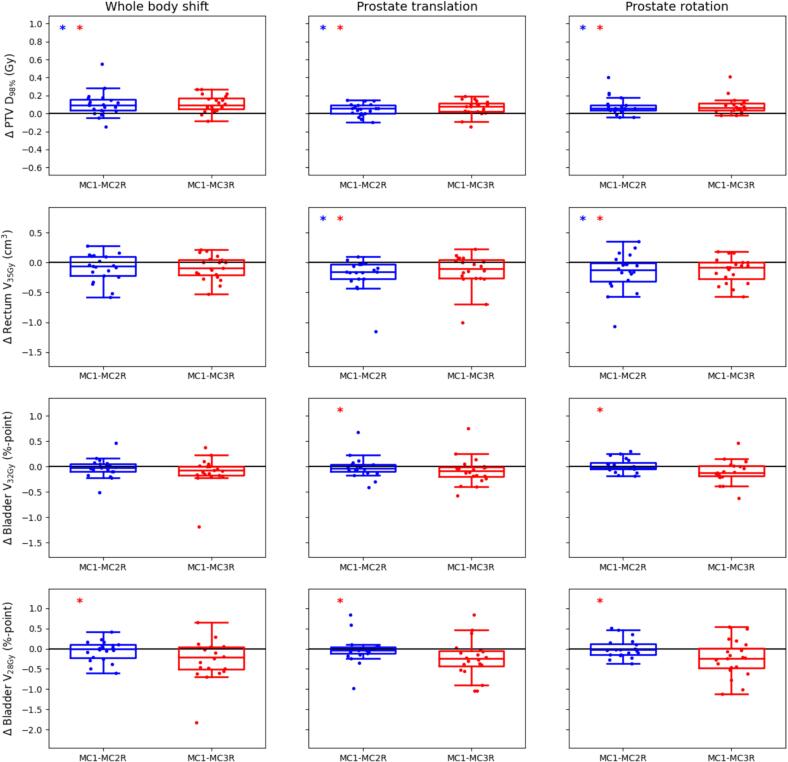
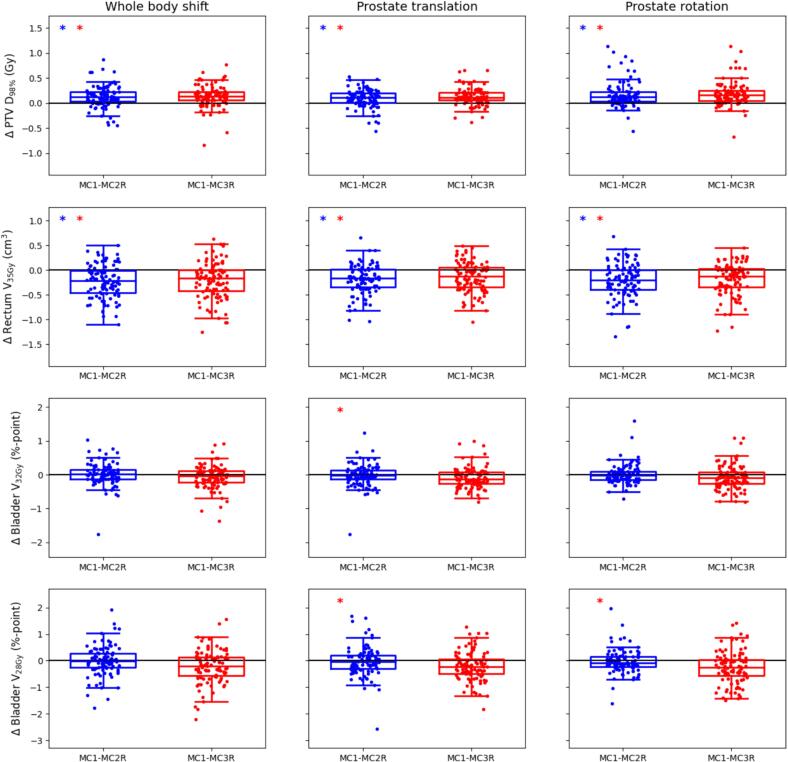
Increasing the statistical uncertainty setting from 1 % to 2-3 % caused an accumulated median target D reduction of 0.1 Gy, with interquartile ranges (IQRs) up to 0.12 Gy. Rectum V increased in median up to 0.16 cm with IQRs up to 0.33 cm. The bladder V and V showed median increases up to 0.24 %-point, with IQRs up to 0.54 %-point. Using 2 % uncertainty reduced calculation times by more than a minute for all modes of variation, with no further time gain when increasing to 3 %.
A 2-3 % MC statistical uncertainty was clinically feasible. Using a 2 % uncertainty setting reduced calculation times at the cost of limited relative dose-volume differences.
基于蒙特卡罗(MC)的剂量计算在放射治疗中被广泛应用,其统计不确定性低,计算准确但速度慢。增加不确定性可加快计算速度,但会降低计算质量。然而,在在线自适应计划中,每次治疗分割都会重新计算剂量,这可能会降低累积计算误差。本研究旨在评估在每日在线计划自适应的背景下,较高的MC统计不确定性所产生的影响。
对于20例前列腺癌患者,模拟了5个分割的每日计划以及三种变化模式:全身刚性平移、前列腺局部刚性平移和前列腺局部刚性旋转。对于每种模式和分割,使用三个MC不确定性值(每个计划1%(标准)、2%和3%)从临床参考计划生成自适应计划。评估累积剂量的剂量体积标准,检查计划的可接受性,并将较高不确定性计划与标准计划进行比较。
将统计不确定性设置从1%增加到2%-3%导致累积中位靶区D降低0.1 Gy,四分位数间距(IQR)高达0.12 Gy。直肠V中位数增加至0.16 cm,IQR高达0.33 cm。膀胱V和V中位数增加至0.24%-点,IQR高达0.54%-点。对于所有变化模式,使用2%的不确定性可将计算时间减少超过1分钟,增加到3%时计算时间没有进一步减少。
2%-3%的MC统计不确定性在临床上是可行的。使用2%的不确定性设置可减少计算时间,但代价是相对剂量体积差异有限。