Plasencia-Rodríguez Chamaida, Martínez-Feito Ana, Novella-Navarro Marta, Pérez De Diego Rebeca, Bonilla Gema, Gehin Johanna Elin, Villalba-Yllán Alejandro, Nuño Laura, Pascual-Salcedo Dora, Nozal Pilar, Almirón Mariana Díaz, Balsa Alejandro
Rheumatology Department, La Paz University Hospital, Madrid, Spain.
Immuno-Rheumatology Research Group, Institute for Health Research (IdiPAZ), Madrid, Spain.
Front Med (Lausanne). 2024 Sep 4;11:1461396. doi: 10.3389/fmed.2024.1461396. eCollection 2024.
The EXXELERATE study revealed poorer clinical outcomes in patients treated with adalimumab (ADL) and baseline rheumatoid factor (RF) above 203 IU/mL. However, responses were similar in patients treated with certolizumab pegol (CZP) regardless of RF levels.
This study investigated the impact of RF levels >203 IU/mL on TNF inhibitors (TNFi) serum levels and the association with secondary nonresponse in RA patients treated with TNFi.
We performed an observational ambispective study with RA patients treated with infliximab (IFX), ADL, or CZP. Patients were stratified according to baseline RF levels: ≤ or >203 IU/mL. After 6 months, serum drug levels and antidrug antibodies were measured, and reasons for discontinuation were collected.
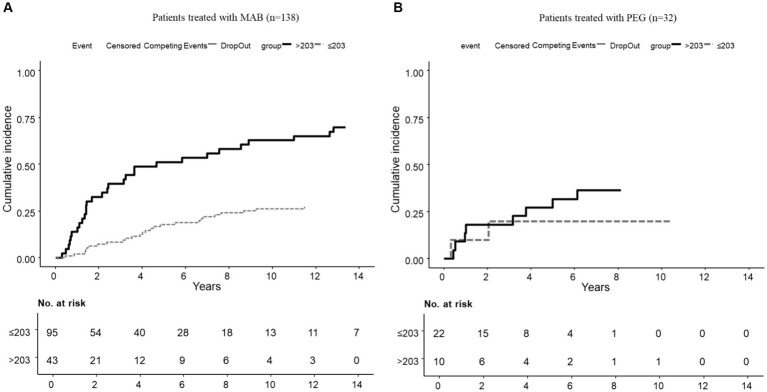
We included 170 RA patients: 90 (53%) received IFX, 48 (28%) ADL, and 32 (19%) CZP. While CZP serum levels did not differ between RF groups at 6 months ( = 0.6), RF levels >203 IU/mL were linked to lower serum drug levels in patients treated with IFX ( = 0.09) or ADL ( = 0.02). Secondary nonresponse was 3.6 times higher in patients with high versus low RF levels in patients under IFX or ADL. However, the reasons for withdrawal were not affected by RF levels in patients treated with CZP.
Baseline RF above 203 IU/mL is associated with lower serum drug levels and an increased risk of discontinuation due to secondary nonresponse in patients treated with IFX or ADL. In contrast, drug levels and clinical outcomes are not significantly impacted by baseline RF levels in patients under CZP.
EXXELERATE研究显示,接受阿达木单抗(ADL)治疗且基线类风湿因子(RF)高于203 IU/mL的患者临床结局较差。然而,无论RF水平如何,接受聚乙二醇化赛妥珠单抗(CZP)治疗的患者反应相似。
本研究调查RF水平>203 IU/mL对肿瘤坏死因子抑制剂(TNFi)血清水平的影响以及与接受TNFi治疗的类风湿关节炎(RA)患者继发无反应的相关性。
我们对接受英夫利昔单抗(IFX)、ADL或CZP治疗的RA患者进行了一项观察性双向研究。患者根据基线RF水平分层:≤或>203 IU/mL。6个月后,测量血清药物水平和抗药物抗体,并收集停药原因。
我们纳入了170例RA患者:90例(53%)接受IFX治疗,48例(28%)接受ADL治疗,32例(19%)接受CZP治疗。虽然6个月时CZP血清水平在RF分组之间无差异(P = 0.6),但RF水平>203 IU/mL与接受IFX(P = 0.09)或ADL(P = 0.02)治疗的患者较低的血清药物水平相关。在接受IFX或ADL治疗的患者中,高RF水平患者的继发无反应是低RF水平患者的3.6倍。然而,接受CZP治疗的患者停药原因不受RF水平影响。
基线RF高于203 IU/mL与接受IFX或ADL治疗的患者较低的血清药物水平以及继发无反应导致停药风险增加相关。相比之下,接受CZP治疗的患者基线RF水平对药物水平和临床结局无显著影响。