RAND Corporation, Washington, District of Columbia, USA.
RAND Corporation, Santa Monica, California, USA.
J Glob Health. 2024 Sep 20;14:04147. doi: 10.7189/jogh.14.04147.
Perinatal depression affects one-third of pregnant women living with HIV (WLH). We examined patterns of treatment response to a novel stepped model of depression care among WLH with perinatal depression in Uganda.
As part of the Maternal Depression Treatment in HIV (M-DEPTH) cluster randomised controlled trial, 191 women were enrolled across four antenatal care clinics assigned to provide stepped care including behavioural and antidepressant therapy (ADT), and another 200 across four clinics assigned to provide usual care. They were assessed for depression severity using the Patient Health Questionnaire (PHQ-9) at enrolment and multiple times over 12 months of follow-up. We used repeated measures latent class analysis (LCA) to identify discrete trajectories of depression symptoms, while multinomial regression analyses measured correlates of class membership.
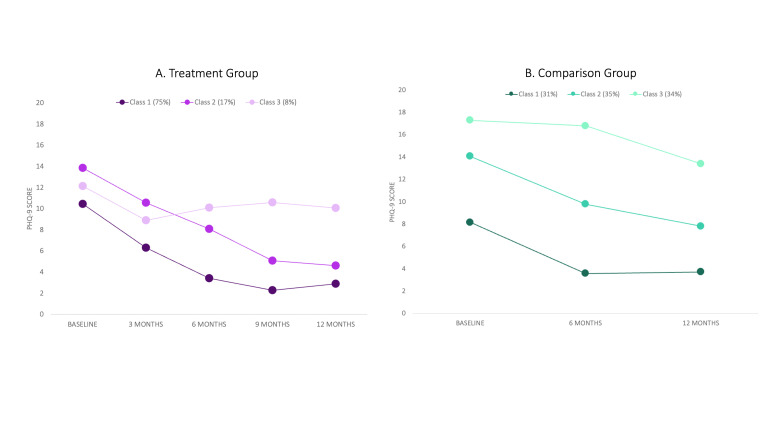
The LCA identified three trajectories among those in the treatment group: mildly depressed individuals who improved (MiD-I) (n = 143, 75%), moderately depressed individuals who improved (MoD-I) (n = 33, 17%), and moderately depressed individuals who remained depressed (MoD-R) (n = 15, 8%). Membership in MiD-I was associated with lower levels of intimate partner violence at baseline (P = 0.04) and month 6 (P < 0.001), and less recent trauma exposure (P = 0.03) at baseline. At month 6, social support was lowest in MoD-R, while the degree of negative problem-solving orientation was highest (both P < 0.001) in this class. The LCA also identified three trajectories among those in the usual care comparison group: mildly depressed (MiD) (n = 62, 31%), moderately depressed (MoD) (n = 71, 35%), and seriously depressed (SiD) (n = 67, 34%), with each experiencing slight improvement. Recent traumas at baseline were highest in SiD (P < 0.001); this group also reported the lowest positive problem-solving orientation and highest negative problem-solving orientation (P < 0.001) at baseline.
Depression symptom trajectories among women with perinatal depression are related to modifiable factors such as problem-solving orientation and interpersonal dynamics, with the latter including intimate partner violence and social support. Most treatment recipients were characterised by trajectories indicating recovery from depression.
ClinicalTrials.Gov (NCT03892915).
围产期抑郁影响了三分之一的感染艾滋病毒的孕妇(WHL)。我们研究了在乌干达,针对 WHL 围产期抑郁的新型阶梯式抑郁护理模式的治疗反应模式。
作为母婴抑郁治疗研究(M-DEPTH)的一部分,191 名妇女在四个产前保健诊所入组,这些诊所被分配提供阶梯式护理,包括行为和抗抑郁治疗(ADT),而另外 200 名妇女在四个诊所入组,提供常规护理。在入组时和 12 个月的随访期间,她们使用患者健康问卷(PHQ-9)评估抑郁严重程度。我们使用重复测量潜在类别分析(LCA)来识别抑郁症状的离散轨迹,同时使用多项回归分析来衡量类别成员的相关性。
治疗组中,LCA 确定了三种轨迹:轻度抑郁患者改善(MiD-I)(n=143,75%),中度抑郁患者改善(MoD-I)(n=33,17%)和中度抑郁患者持续抑郁(MoD-R)(n=15,8%)。MiD-I 组的基线(P=0.04)和第 6 个月(P<0.001)的亲密伴侣暴力程度较低,近期创伤暴露较少(P=0.03)。在第 6 个月,MoD-R 的社会支持最低,而该类别的负面问题解决取向程度最高(均 P<0.001)。LCA 还在常规护理对照组中确定了三种轨迹:轻度抑郁(MiD)(n=62,31%),中度抑郁(MoD)(n=71,35%)和严重抑郁(SiD)(n=67,34%),每个轨迹都有轻微改善。基线时最近的创伤在 SiD 组中最高(P<0.001);该组报告的积极问题解决取向最低,消极问题解决取向最高(均 P<0.001)。
围产期抑郁妇女的抑郁症状轨迹与可改变的因素有关,如问题解决取向和人际关系动态,后者包括亲密伴侣暴力和社会支持。大多数治疗对象的特征是表明从抑郁中恢复的轨迹。
ClinicalTrials.Gov(NCT03892915)。