Department of Anesthesiology, Perioperative and Pain Medicine, Nanjing First Hospital, Nanjing Medical University, Nanjing, 210006, China.
J Cardiothorac Surg. 2024 Sep 20;19(1):537. doi: 10.1186/s13019-024-03064-4.
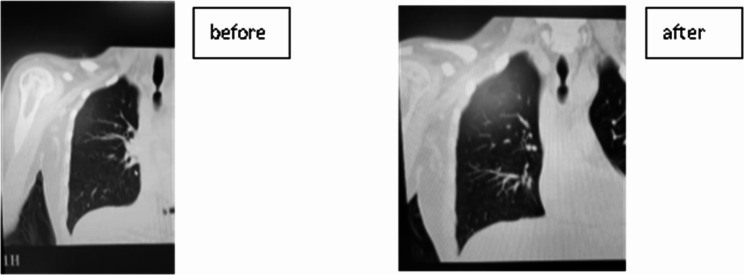
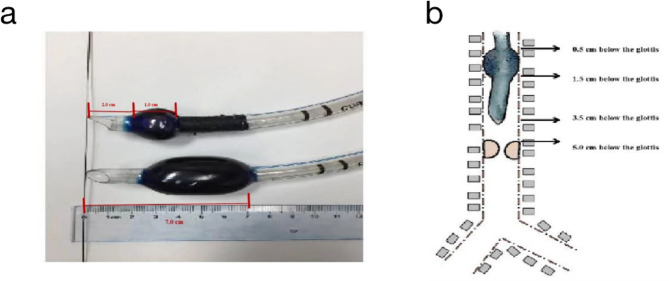
Both anaesthesiologists and surgeons experience challenges in managing airway stenosis and scar contracture in the face and neck. Herein, we report the case of a 38-year-old woman (BMI 23.1 kg/m, third-degree burns covering 40% of her body, an American Society of Anaesthesiologists physical status III) with an unusual case of airway constriction. This patient had a predictable difficult airway (mouth opening of 2 cm, bilateral nostril scar hyperplasia, Mallampatti score III, scarring of the head and neck, and severe tracheal stenosis). Tracheal stenosis measuring 5.5 mm in width as observed 8 cm below the glottis, and the bronchoscope could not pass through it. After two failed attempts at laryngeal mask insertion, we decided to instead insert a custom-made tracheal tube under the guidance of a fiberoptic bronchoscope. The operation was successful, and the patient was transferred to the intensive care unit (ICU).
麻醉师和外科医生在处理头颈部气道狭窄和疤痕挛缩时都面临挑战。在此,我们报告了一例 38 岁女性(BMI 23.1kg/m,三度烧伤面积 40%,美国麻醉医师协会身体状况 III 级)气道狭窄的不寻常病例。该患者存在可预测的困难气道(张口度 2cm,双侧鼻孔疤痕增生,Mallampatti 评分 III 级,头颈部疤痕形成,严重的气管狭窄)。在声门下 8cm 处观察到气管狭窄处的宽度为 5.5mm,支气管镜无法通过。在两次尝试喉罩插入失败后,我们决定在纤维支气管镜引导下插入定制的气管导管。手术成功,患者被转至重症监护病房(ICU)。