Fischer Stefanie, Gillessen Silke, Stalder Odile, Terbuch Angelika, Cathomas Richard, Schmid Florian A, Zihler Deborah, Müller Beat, Fankhauser Christian D, Hirschi-Blickenstorfer Anita, Kluth Luis Alex, Seifert Bettina, Templeton Arnoud J, Mingrone Walter, Ufe Mark-Peter, Fischer Natalie, Beyer Jörg, Woelky Regina, Omlin Aurelius, Vogl Ursula, Hoppe Katharina, Kamradt Jörn, Rothschild Sacha I, Rothermundt Christian
Department of Medical Oncology and Haematology, Cantonal Hospital St. Gallen, St. Gallen, Switzerland.
Oncology Institute of Southern Switzerland, Ente Ospedaliero Cantonale, Bellinzona, Switzerland.
Eur Urol Open Sci. 2024 Sep 11;68:68-74. doi: 10.1016/j.euros.2024.08.008. eCollection 2024 Oct.
Follow-up for patients with testicular cancer should ensure early detection of relapses. Optimal schedules and minimum requirements for cross-sectional imaging are not clearly defined, and guideline recommendations differ. Our aim was to analyse the clinical impact of different imaging modalities for detection of relapse in a large prospective cohort (Swiss Austrian German Testicular Cancer Cohort Study, SAG TCCS).
Patients with seminoma or nonseminoma were prospectively enrolled between January 2014 and February 2023 after initial treatment ( = 1175). Follow-up according to the study schedule was individualised for histology and disease stage. Only patients who had received primary treatment were considered. We analysed the total number of imaging modalities and scans identifying relapse and the timing of relapse.
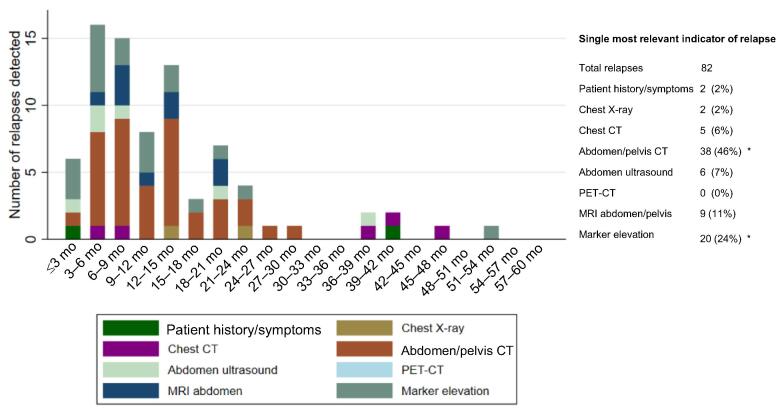
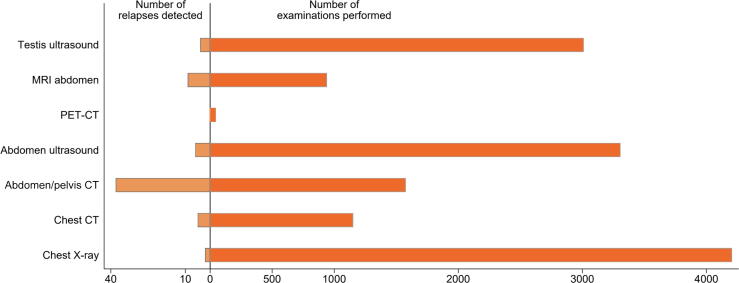
We analysed data for 1006 patients (64% seminoma, 36% nonseminoma); 76% had stage I disease. Active surveillance was the most frequent management strategy (65%). Recurrence occurred in 82 patients, corresponding to a 5-yr relapse-free survival rate of 90.1% (95% confidence interval 87.7-92.1%). Median follow-up for patients without relapse was 38.4 mo (interquartile range 21.6-61.0). Cross-sectional imaging of the abdomen was the most important indicator of relapse 57%, abdominal CT accounting for 46% and MRI for 11%. Marker elevation indicated relapse in 24% of cases. Chest X-ray was the least useful modality, indicating relapse in just 2% of cases.
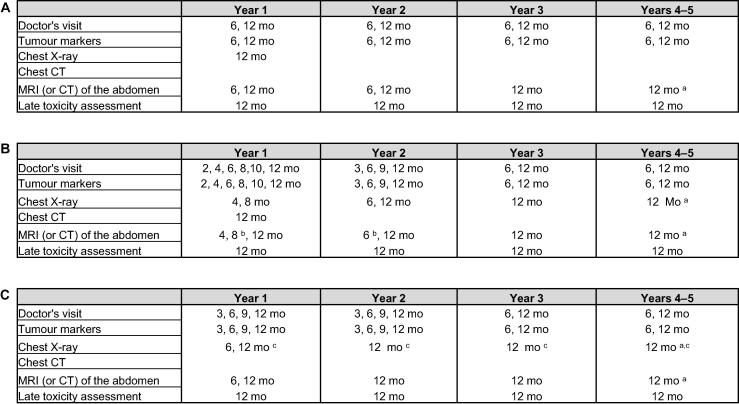
On the basis of findings from our prospective register, we have adapted a follow-up schedules with an emphasis on abdominal imaging and a reduction in chest X-rays. This schedule might provide additional guidance for clinicians and will be prospectively evaluated as SAG TCCS continues to enrol patients.
We analysed the value of different types of imaging scans for detection of relapse of testicular cancer. We used our findings to propose an optimum follow-up schedule for patients with testicular cancer.
睾丸癌患者的随访应确保早期发现复发情况。目前,对于横断面成像的最佳方案和最低要求尚无明确定义,指南建议也存在差异。我们的目的是分析在一个大型前瞻性队列研究(瑞士-奥地利-德国睾丸癌队列研究,SAG TCCS)中,不同成像方式对复发检测的临床影响。
2014年1月至2023年2月期间,对接受初始治疗后的精原细胞瘤或非精原细胞瘤患者进行前瞻性入组(n = 1175)。根据研究方案进行的随访针对组织学和疾病分期进行了个体化安排。仅考虑接受过初始治疗的患者。我们分析了识别复发的成像方式和扫描的总数以及复发时间。
我们分析了1006例患者的数据(64%为精原细胞瘤,36%为非精原细胞瘤);76%的患者为I期疾病。主动监测是最常用的管理策略(65%)。82例患者出现复发,5年无复发生存率为90.1%(95%置信区间87.7 - 92.1%)。无复发患者的中位随访时间为38.4个月(四分位间距21.6 - 61.0)。腹部横断面成像为复发的最重要指标(57%),腹部CT占46%,MRI占11%。标志物升高在24%的病例中提示复发。胸部X线是最无用的检查方式,仅在2%的病例中提示复发。
基于我们前瞻性登记研究的结果,我们调整了随访方案,重点是腹部成像并减少胸部X线检查。该方案可能为临床医生提供额外指导,并将在SAG TCCS继续招募患者时进行前瞻性评估。
我们分析了不同类型成像扫描对睾丸癌复发检测的价值。我们利用研究结果为睾丸癌患者提出了最佳随访方案。