Department of Pediatrics, Indiana University School of Medicine, Indianapolis.
Department of Preventive Medicine, University of Tennessee Health Science Center, Memphis.
JAMA Netw Open. 2024 Sep 3;7(9):e2435416. doi: 10.1001/jamanetworkopen.2024.35416.
Prescribing medications for opioid use disorders (MOUD), including buprenorphine, naltrexone, and methadone, to adolescents remains an underused evidence-based strategy for reducing harms associated with opioid use.
To identify potential associations between clinician- and community-level characteristics regarding clinicians' self-reported willingness to prescribe MOUD to adolescents.
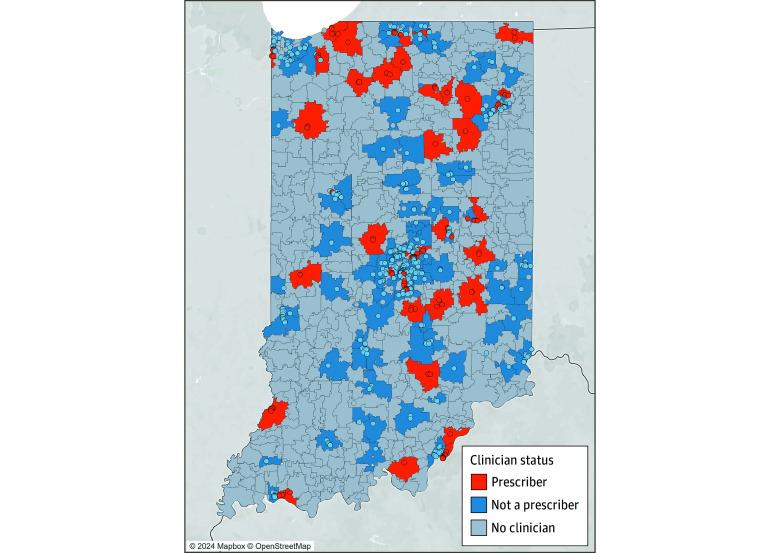
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included a phone survey of Indiana clinicians and spatial analysis of community-level characteristics. Clinicians were eligible for inclusion in analyses if actively providing health care and listed on the Buprenorphine Practitioner Locator website, a publicly available national registry of clinicians possessing a waiver to legally prescribe buprenorphine (ie, waivered clinicians).
Community-level characteristics, including total population, rurality or urbanicity, percentage with incomes below the federal poverty line, and racial or ethnic makeup.
Clinicians were asked about their willingness to prescribe MOUD to adolescents younger than 18 years if clinically indicated. Responses were recorded as no, yes, or yes with conditions.
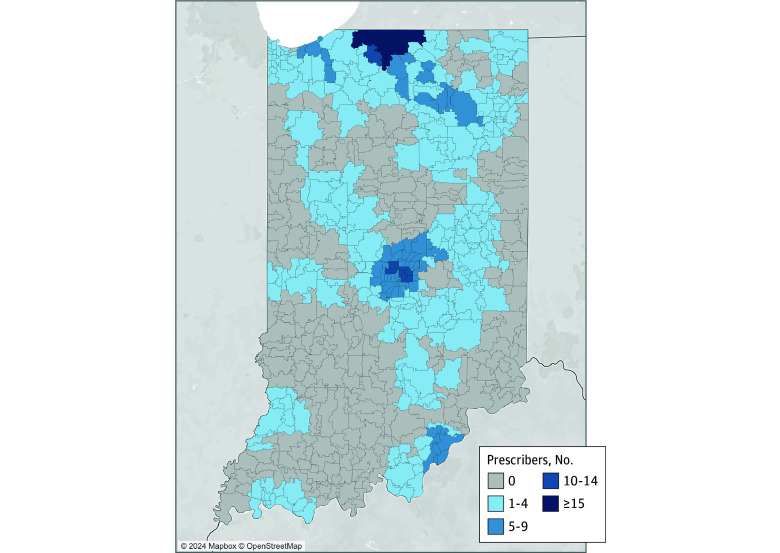
Among the 871 clinicians listed on the website as of July 2022, 832 were eligible for inclusion and contacted by phone. Among waivered clinicians, 759 (91.2%) reported being unwilling to prescribe MOUD to adolescents, 73 clinicians (8.8%) reported willingness to prescribe MOUD to adolescents, and only 24 (2.9%) would do so without conditions. A multivariable logistic regression model including spatially lagged community-level variables showed that, among areas with waivered clinicians, clinicians practicing in more populated areas were significantly less likely to prescribe to adolescents (β = 0.65; 95% CI, 0.49-0.87; P = .003). Similarly, those in more rural areas were significantly more likely to prescribe to adolescents (β = 1.27; 95% CI, 1.02-1.58; P = .03). Variation in clinician willingness to prescribe was not explained by other community-level characteristics. Among all waivered clinicians, advanced practice clinicians were less likely than physicians to report willingness to prescribe (β = 0.58; 95% CI, 0.35-0.97; P = .04), as were physicians without any specialty training relevant to MOUD prescribing when compared with family medicine clinicians (β = 0.40; 95% CI, 0.18-0.89; P = .03). A small subgroup of waivered clinicians had training in pediatrics (13 clinicians [1.6%]), and none were willing to prescribe MOUD to adolescents.
From this cross-sectional study, it appears that Indiana adolescents continued to face gaps in access to MOUD treatment, despite its well-established efficacy. Programs that support primary care practitioners, including family medicine clinicians and pediatricians, in safe and appropriate use of MOUD in adolescents may bridge these gaps.
为阿片类药物使用障碍(MOUD)开处方,包括丁丙诺啡、纳曲酮和美沙酮,对于青少年来说,仍然是一种未被充分利用的基于证据的策略,可以减少与阿片类药物使用相关的危害。
确定临床医生和社区层面特征与临床医生自我报告的为青少年开 MOUD 的意愿之间的潜在关联。
设计、地点和参与者:这是一项横断面研究,包括对印第安纳州临床医生的电话调查和社区层面特征的空间分析。如果临床医生积极提供医疗保健服务,并在 Buprenorphine Practitioner Locator 网站上列出,这是一个公开的全国临床医生名册,拥有合法开处丁丙诺啡的豁免权(即豁免临床医生),则有资格参与分析。
社区层面的特征,包括总人口、农村或城市、收入低于联邦贫困线的百分比以及种族或民族构成。
临床医生被问及如果临床上有需要,他们是否愿意为 18 岁以下的青少年开 MOUD。答复记录为否、是或有条件的是。
在截至 2022 年 7 月网站上列出的 871 名临床医生中,有 832 名符合条件并通过电话联系。在豁免临床医生中,759 名(91.2%)报告不愿意为青少年开 MOUD,73 名(8.8%)报告愿意为青少年开 MOUD,只有 24 名(2.9%)愿意无条件开处方。包括空间滞后社区层面变量的多变量逻辑回归模型显示,在有豁免临床医生的地区,在人口较多的地区执业的临床医生开处方给青少年的可能性显著降低(β=0.65;95%CI,0.49-0.87;P=0.003)。同样,在农村地区执业的临床医生开处方给青少年的可能性显著增加(β=1.27;95%CI,1.02-1.58;P=0.03)。临床医生开处方的意愿差异不能用其他社区层面特征来解释。在所有豁免临床医生中,与医生相比,高级实践临床医生报告愿意开处方的可能性较小(β=0.58;95%CI,0.35-0.97;P=0.04),与家庭医学临床医生相比,没有任何与 MOUD 开处方相关的专业培训的医生报告愿意开处方的可能性也较小(β=0.40;95%CI,0.18-0.89;P=0.03)。一小部分豁免临床医生接受过儿科培训(13 名医生[1.6%]),但他们都不愿意为青少年开 MOUD。
从这项横断面研究来看,印第安纳州的青少年似乎仍然面临 MOUD 治疗机会不足的问题,尽管其疗效已得到充分证实。支持初级保健医生,包括家庭医学临床医生和儿科医生,在青少年中安全和适当使用 MOUD 的项目可能会弥合这些差距。