Adatia Adil, Boursiquot Jean-Nicolas, Goodyear Dawn, Kalicinsky Chrystyna, Kanani Amin, Waserman Susan, Nguyen Michelle M L, Wadhwa Abhinav, Weiss Jessica, El-Zoeiby Ahmed, Betschel Stephen
Alberta Health Services, University of Alberta, Edmonton, AB, Canada.
CHU de Québec, Université Laval, Québec, QC, Canada.
Allergy Asthma Clin Immunol. 2024 Sep 27;20(1):50. doi: 10.1186/s13223-024-00910-x.
Hereditary angioedema with normal C1-inhibitor function (HAE nC1-INH) and idiopathic angioedema of unknown etiology (AE-UNK) are rare conditions that cause recurrent subcutaneous and submucosal swelling. The characteristics and clinical outcomes of patients with these conditions in Canada have not been studied.
The aim of this study was to extract real-world evidence from the electronic health records of patients with HAE nC1-INH or AE-UNK who were managed in selected practices of Canadian HAE-treating specialist physicians between 01-Jan-2012 and 01-Jan-2022, to examine case numbers, treatment, clinical outcomes, and healthcare utilization.
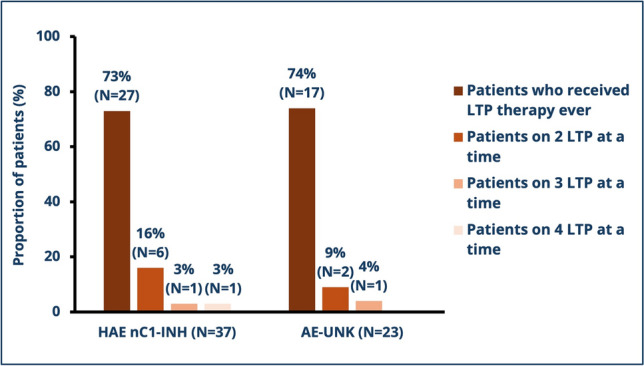
Of 60 patients (37 with HAE nC1-INH, 23 with AE-UNK), median (range) age at symptom onset was 21.5 (5.0-57.0) and 23.0 (10.0-54.0) years, respectively. Time to diagnosis from onset of symptoms was 7.0 (0.0-43.0) and 2.0 (- 10.0 to 50.0) years. Significant differences were observed in terms of the predominant triggers for angioedema attacks between patients with HAE nC1-INH and AE-UNK: stress (65% vs. 26%, p = 0.007) and estrogen therapy (35% vs. 9%, p = 0.031). Before diagnosis, most patients received antihistamines (50% of HAE nC1-INH and 61% of AE-UNK patients). Post-diagnosis, 73% and 74% of HAE nC1-INH and AE-UNK patients received long-term prophylaxis (LTP), with the most common LTP treatments being subcutaneous pdC1-INH (43% of HAE nC1-INH patients and 39% of AE-UNK patients) and tranexamic acid (41% of HAE nC1-INH patients and 35% of AE-UNK patients). Of patients with HAE nC1-INH, and patients with AE-UNK, 22% and 13%, respectively, were taking more than one LTP treatment concurrently. Before HAE treatment initiation, significantly fewer patients with AE-UNK compared to patients with HAE nC1-INH had angioedema attacks affecting their extremities (13% vs. 38%, p = 0.045) and GI system (22% vs. 57%, p = 0.015). In the three months following treatment initiation, patients with AE-UNK experienced significantly fewer angioedema attacks compared to patients with HAE nC1-INH (median 2.0 attacks [0.0-48.0] vs. 6.0 attacks [0.0-60.0], p = 0.044). Additionally, fewer patients with AE-UNK compared to HAE nC1-INH experienced attacks affecting their GI system (26% vs. 57%, p = 0.032). Attack duration and frequency significantly decreased for patients with HAE nC1-INH from a median of 1.00 day (range: 0.00-7.00) to 0.29 day (range: 0.02-4.00; p = 0.001) and from 10.50 attacks (range: 0.00-90.00) to 6.00 attacks (range: 0.00-60.00; p = 0.004) in the three months following HAE treatment initiation.
Using Canadian real-world evidence, these data demonstrate differing clinical trajectories between patients with HAE nC1-INH and AE-UNK, including diagnostic delays, varied attack characteristics, treatment responses and healthcare utilization. Despite treatment response, many patients still experienced frequent angioedema attacks. These results suggest an unmet need for treatment guidelines and therapies specifically for patients with HAE nC1-INH and AE-UNK and better understanding of the pathophysiology accounting for the reported differences between the two.
C1抑制物功能正常的遗传性血管性水肿(HAE nC1-INH)和病因不明的特发性血管性水肿(AE-UNK)是导致反复皮下和黏膜下肿胀的罕见病症。加拿大患有这些病症的患者的特征和临床结局尚未得到研究。
本研究的目的是从2012年1月1日至2022年1月1日在加拿大遗传性血管性水肿治疗专科医生的选定诊所接受治疗的HAE nC1-INH或AE-UNK患者的电子健康记录中提取真实世界证据,以检查病例数量、治疗、临床结局和医疗保健利用情况。
在60例患者中(37例HAE nC1-INH,23例AE-UNK),症状发作时的中位(范围)年龄分别为21.5(5.0 - 57.0)岁和23.0(10.0 - 54.0)岁。从症状发作到诊断的时间分别为7.0(0.0 - 43.0)年和2.0(-10.0至50.0)年。在HAE nC1-INH患者和AE-UNK患者的血管性水肿发作的主要触发因素方面观察到显著差异:压力(65%对26%,p = 0.007)和雌激素治疗(35%对9%,p = 0.031)。在诊断之前,大多数患者接受了抗组胺药治疗(HAE nC1-INH患者的50%和AE-UNK患者的61%)。诊断后,73%的HAE nC1-INH患者和74%的AE-UNK患者接受了长期预防(LTP),最常见的LTP治疗是皮下注射pdC1-INH(HAE nC1-INH患者的43%和AE-UNK患者的39%)和氨甲环酸(HAE nC1-INH患者的41%和AE-UNK患者的35%)。在HAE nC1-INH患者和AE-UNK患者中,分别有22%和13%的患者同时接受多种LTP治疗。在开始HAE治疗之前,与HAE nC1-INH患者相比,AE-UNK患者中血管性水肿发作影响其四肢的患者明显更少(13%对38%,p = 0.045),影响胃肠道系统的患者也更少(22%对57%,p = 0.015)。在开始治疗后的三个月内,与HAE nC1-INH患者相比,AE-UNK患者经历的血管性水肿发作明显更少(中位2.0次发作[0.0 - 48.0]对6.0次发作[0.0 - 60.0],p = 0.044)。此外,与HAE nC1-INH患者相比,AE-UNK患者中经历影响其胃肠道系统发作的患者更少(26%对57%,p = 0.032)。HAE nC1-INH患者的发作持续时间和频率在开始HAE治疗后的三个月内从中位1.oo天(范围:0.00 - 7.00)显著降至0.29天(范围:0.02 - 4.00;p = 0.001),发作次数从10.50次(范围:0.00 - 90.00)降至6.00次(范围:0.00 - 60.00;p = 0.