School of Medicine, Louisiana State University Health Science Center at New Orleans, New Orleans, LA, 70112, USA.
School of Medicine, Louisiana State University Health Science Center at Shreveport, 1501 Kings Highway, Shreveport, LA, 71103, USA.
Adv Ther. 2023 Mar;40(3):814-827. doi: 10.1007/s12325-022-02401-0. Epub 2023 Jan 7.
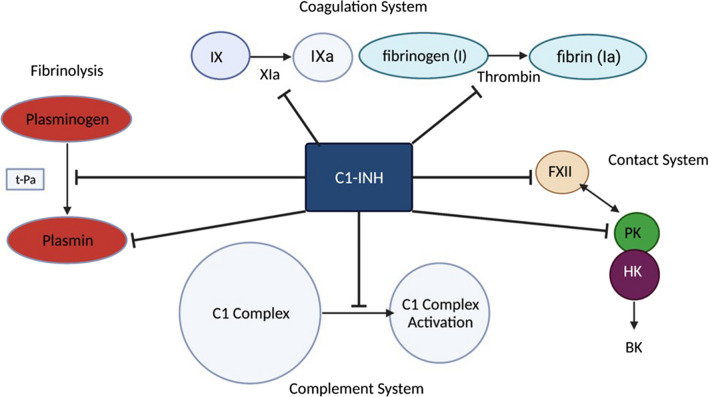
Hereditary angioedema (HAE) is an autosomal dominant disorder caused by a mutation in the C1 esterase inhibitor gene. HAE affects 1/50,000 people worldwide. Three main types of HAE exist: type I, type II, and type III. Type I is characterized by a deficiency in C1-INH. C1-INH is important in the coagulation complement, contact systems, and fibrinolysis. Most HAE cases are type I. Type I and II HAE result from a mutation in the SERPING1 gene, which encodes C1-INH. Formally known as type III HAE is typically an estrogen-dependent or hereditary angioedema with normal C1-INH activity. Current guidelines now recommend subdividing hereditary angioedema with normal C1 esterase inhibitor gene (HAE-nl-C1-INH formerly known as HAE type III) based on underlying mutations such as in kininogen-1 (HAE-KNG1), plasminogen gene (PLG-HAE), myoferlin gene mutation (MYOF-HAE), heparan sulfate-glucosamine 3-sulfotransferase 6 (HS3ST6), mutation in Hageman factor (factor XII), and in angiopoietin-1 (HAE-ANGPT-1). The clinical presentation of HAE varies between patients, but it usually presents with nonpitting angioedema and occasionally abdominal pain. Young children are typically asymptomatic. Those affected by HAE usually present with symptoms in their early 20s. Symptoms can arise as a result of stress, infection, or trauma. Laboratory testing shows abnormal levels of C1-INH and high levels of bradykinin. C4 and D-dimer levels can also be monitored if an acute HAE attack is suspected. Acute treatment of HAE can include IV infusions of C1-INH, receptor antagonists, and kallikrein inhibitors. Short- and long-term prophylaxis can also be administered to patients with HAE. First-line therapies for long-term prophylaxis also include IV infusion of C1-INH. This review aims to thoroughly understand HAE, its clinical presentation, and how to treat it.
遗传性血管性水肿(HAE)是一种常染色体显性遗传疾病,由 C1 酯酶抑制剂基因的突变引起。HAE 影响全球每 50,000 人中的 1 人。存在三种主要类型的 HAE:I 型、II 型和 III 型。I 型的特征是 C1-INH 缺乏。C1-INH 在凝血补体、接触系统和纤维蛋白溶解中很重要。大多数 HAE 病例为 I 型。I 型和 II 型 HAE 是由 SERPING1 基因突变引起的,该基因编码 C1-INH。正式称为 III 型 HAE 通常是一种雌激素依赖性或遗传性血管性水肿,C1-INH 活性正常。目前的指南现在建议根据潜在的突变(如激肽原-1 [HAE-KNG1]、纤溶酶原基因 [PLG-HAE]、肌抑素基因突变 [MYOF-HAE]、硫酸乙酰肝素-葡糖胺 3-硫酸转移酶 6 [HS3ST6]、因子 XII 中的突变和血管生成素-1 [HAE-ANGPT-1])对正常 C1 酯酶抑制剂基因(HAE-nl-C1-INH 以前称为 HAE 型 III)的遗传性血管性水肿进行细分。HAE 的临床表现因患者而异,但通常表现为非凹陷性血管性水肿,偶尔伴有腹痛。幼儿通常无症状。受 HAE 影响的人通常在 20 多岁时出现症状。症状可能因压力、感染或创伤而出现。实验室检查显示 C1-INH 水平异常和缓激肽水平升高。如果怀疑发生急性 HAE 发作,也可以监测 C4 和 D-二聚体水平。HAE 的急性治疗可包括 C1-INH 的静脉输注、受体拮抗剂和激肽释放酶抑制剂。也可以向 HAE 患者给予短期和长期预防措施。长期预防的一线治疗方法还包括 C1-INH 的静脉输注。本综述旨在深入了解 HAE 的临床表现以及如何治疗它。