Nygaard Hanne, Kamper Rikke S, Nielsen Finn E, Hansen Sofie K, Hansen Pernille, Wejse Miriam R, Pressel Eckart, Rasmussen Jens, Suetta Charlotte, Ekmann Anette
Department of Emergency Medicine, Copenhagen University Hospital, Bispebjerg and Frederiksberg, Copenhagen, Denmark.
CopenAge, Copenhagen Center for Clinical Age Research, University of Copenhagen, Copenhagen, Denmark.
Eur Geriatr Med. 2024 Dec;15(6):1899-1908. doi: 10.1007/s41999-024-01062-2. Epub 2024 Sep 28.
To examine the prognostic accuracy of the Clinical Frailty Scale (CFS) and Braden Scale (BS) separately and combined for 90-day mortality. Furthermore, to examine the effect of frailty on mortality depending on different levels of the Braden score.
The study included acutely admitted medical patients ≥ 65 years. We used an optimum cutoff for CSF and BS at ≥ 4 and ≤ 19, respectively. CFS categorized frailty as Non-frail (< 4), Frail (4-5), and Severely frail (> 5). Prognostic accuracy was estimated by the area under the receiver operating characteristic curves (AUROC) with 95% confidence intervals (CI). Cox regression analysis was used to compute the adjusted hazard ratio (aHR) for mortality.
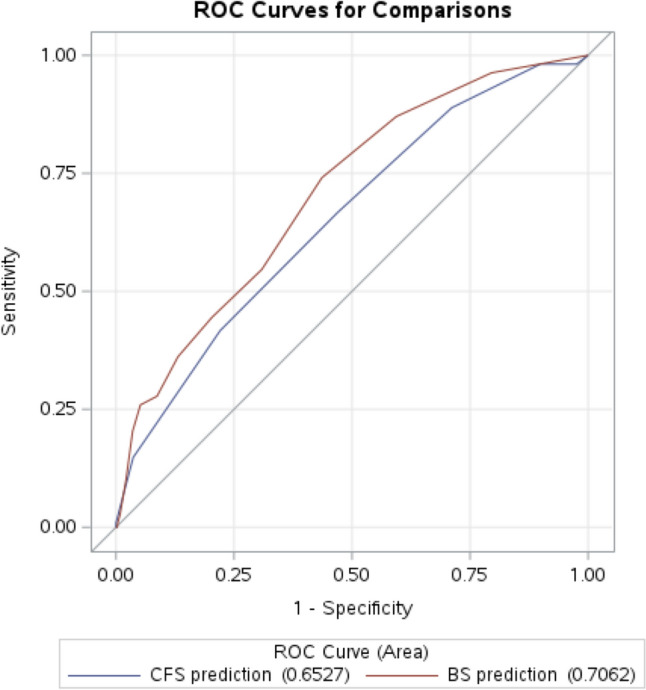
The mean age among 901 patients (54% female) was 79 years. The AUROC for CFS and BS was 0.65 (CI95% 0.60-0.71) and 0.71 (CI95% 0.66-0.76), respectively. aHR for mortality of CFS ≥ 4, BS ≤ 19, and combined were 2.3 (CI95% 1.2-4.2), 1.9 (CI95% 1.3-2.9), and 1.9 (CI95% 1.3-2.8), respectively. For BS > 19, the aHR for mortality was 2.2 (CI95% 1.0-4.8) and 3.5 (CI95% 1.4-8.6) for 'frail' and 'severely frail', respectively. aHR for BS ≤ 19 was 1.1 (CI95% 0.4-3.2) and 1.3 (CI95% 0.5-3.7) for 'frail' and 'severely frail', respectively.
Although CFS and BS were associated with 90-day mortality among older acutely admitted medical patients, the prognostic accuracy was poor-to-moderate, and the combination of CFS and BS did not improve the prognostic accuracy. However, the hazard of mortality across different levels of frailty groups were particularly increased among patients with high BS scores.
分别检验临床衰弱量表(CFS)和Braden量表(BS)对90天死亡率的预后准确性,并检验二者联合使用时的预后准确性。此外,根据Braden评分的不同水平,检验衰弱对死亡率的影响。
该研究纳入了年龄≥65岁的急性入院内科患者。我们分别将CFS和BS的最佳截断值设定为≥4和≤19。CFS将衰弱分为非衰弱(<4)、衰弱(4 - 5)和严重衰弱(>5)。通过受试者工作特征曲线下面积(AUROC)及95%置信区间(CI)来评估预后准确性。采用Cox回归分析计算死亡率的调整风险比(aHR)。
901例患者(54%为女性)的平均年龄为79岁。CFS和BS的AUROC分别为0.65(95%CI 0.60 - 0.71)和0.71(95%CI 0.66 - 0.76)。CFS≥4、BS≤19以及二者联合时的死亡率aHR分别为2.3(95%CI 1.2 - 4.2)、1.9(95%CI 1.3 - 2.9)和1.9(95%CI 1.3 - 2.8)。对于BS>19的情况,“衰弱”和“严重衰弱”的死亡率aHR分别为2.2(95%CI 1.0 - 4.8)和3.5(95%CI 1.4 - 8.6)。对于BS≤19的情况,“衰弱”和“严重衰弱”的死亡率aHR分别为1.1(95%CI 0.4 - 3.2)和1.3(95%CI 0.5 - 3.7)。
虽然CFS和BS与急性入院老年内科患者的90天死亡率相关,但预后准确性为中等到较差,且CFS和BS联合使用并未提高预后准确性。然而,在Braden评分较高的患者中,不同衰弱组别的死亡风险尤其增加。