Diederich Joé, Müller Kurt E
Center for General, Clinical Environmental and Functional Medicine, Colmar-Berg, Luxembourg.
University of Luxembourg, Faculty of Science, Technology and Medicine, Department of Life Sciences and Medicine, Esch-sur-Alzette, Luxembourg.
Pragmat Obs Res. 2024 Sep 24;15:165-172. doi: 10.2147/POR.S479124. eCollection 2024.
Endodontic inflammation typically results from root canal infections and sensitizations to filling materials after root canal treatment (RCT), potentially leading to systemic inflammation and disease. We therefore aimed to characterize the inflammatory alterations after RCT as well as the inflammatory molecule levels following tooth extraction or renewed RCT.
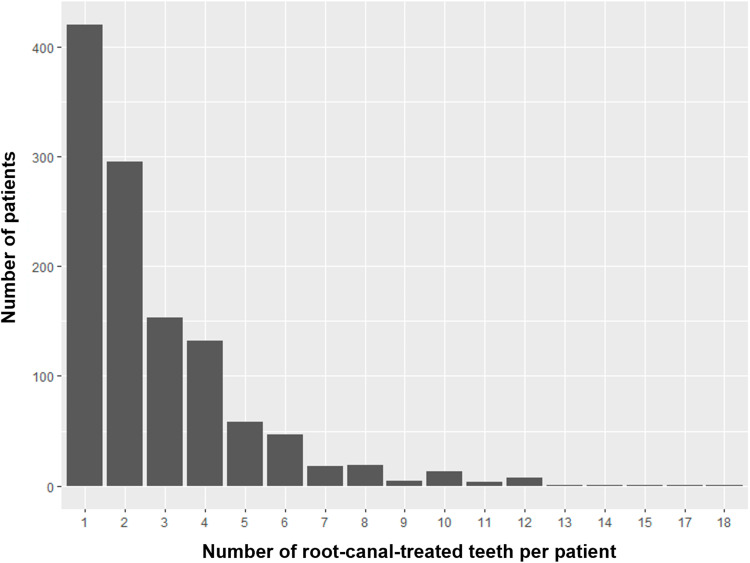
All (a total of 2585) walk-in patients with or without RCT history were included in this retrospective study. During the 3-year observation period, blood levels of RANTES/CCL5 (regulated on activation, normal T-cell expressed and secreted/chemotactic cytokine ligand 5), C-reactive protein (CRP), tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ), and interleukin-10 (IL-10) were measured before and after tooth extraction or renewed RCT. Control patients did not undergo any dental treatment.
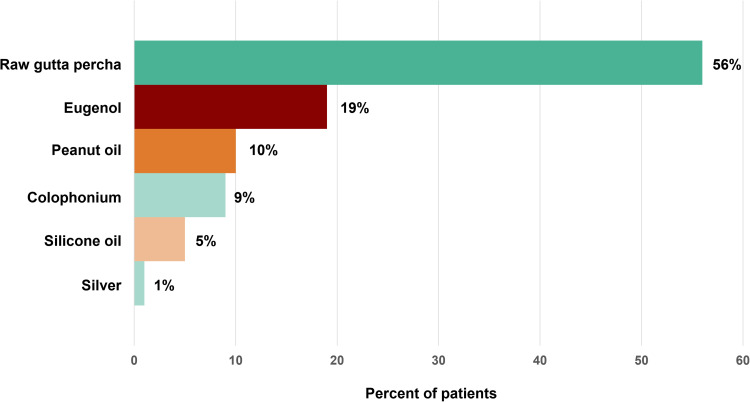
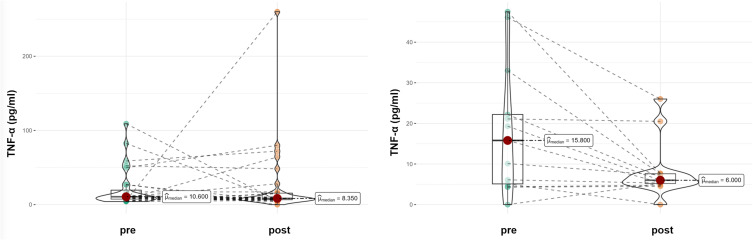
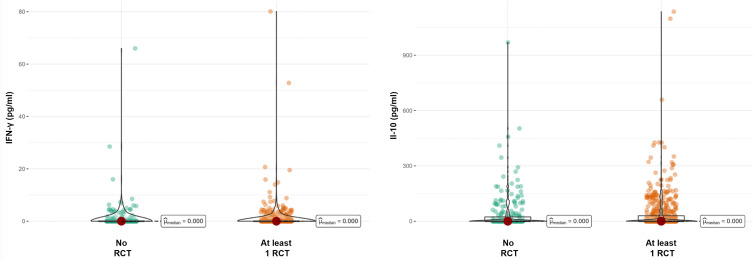
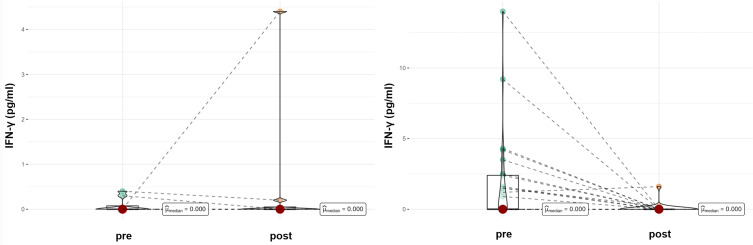
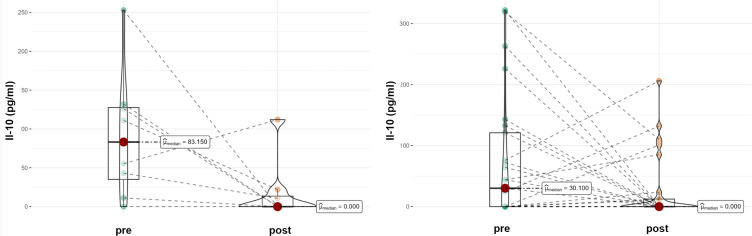
A total 49.38% of patients had a history of at least one RCT. In RCT patients, RANTES/CCL5 values were significantly reduced by both tooth extraction (p=0.03) and renewed dental RCT (p=0.038), while a non-significant increase was observed in untreated patients. TNF-α levels were reduced by tooth extraction (p=0.014) but not by renewed RCT and no intervention. CRP levels were not significantly changed by either treatment. Tooth extraction significantly lowered IFN-γ levels (p=0.003), while in control patients, IFN-γ levels did not change. IL-10 levels were non-significantly reduced by tooth extraction (p=0.061). In a subcohort of RCT patients, the lymphocyte transformation test revealed an allergic reaction to at least one of the root filling materials in 39.46% of patients, with raw gutta percha (56%) and eugenol (19%) being frequent triggers.
Here, we demonstrate the involvement of root-treated teeth in inflammatory processes, as tooth extraction and renewed RCT could significantly reduce individual cytokine levels. Our data support the use of biomarkers for in vivo monitoring of treatment success.
牙髓炎症通常由根管感染以及根管治疗(RCT)后对充填材料的敏感化引起,可能导致全身炎症和疾病。因此,我们旨在描述RCT后的炎症改变以及拔牙或再次RCT后的炎症分子水平。
本回顾性研究纳入了所有(共2585例)有或无RCT病史的门诊患者。在3年观察期内,在拔牙或再次RCT前后测量RANTES/CCL5(活化调节正常T细胞表达和分泌/趋化细胞因子配体5)、C反应蛋白(CRP)、肿瘤坏死因子-α(TNF-α)、干扰素-γ(IFN-γ)和白细胞介素-10(IL-10)的血药浓度。对照患者未接受任何牙科治疗。
共有49.38%的患者有至少一次RCT病史。在RCT患者中,拔牙(p=0.03)和再次进行牙科RCT(p=0.038)均使RANTES/CCL5值显著降低,而未治疗患者中观察到非显著升高。TNF-α水平通过拔牙降低(p=0.014),但再次RCT和无干预未使其降低。两种治疗方式均未使CRP水平发生显著变化。拔牙显著降低了IFN-γ水平(p=0.003),而在对照患者中,IFN-γ水平未改变。拔牙使IL-10水平非显著降低(p=0.061)。在RCT患者的一个亚组中,淋巴细胞转化试验显示39.46%的患者对至少一种根管充填材料有过敏反应,其中生橡胶(56%)和丁香酚(19%)是常见诱因。
在此,我们证明了根管治疗后的牙齿参与炎症过程,因为拔牙和再次RCT可显著降低个体细胞因子水平。我们的数据支持使用生物标志物对治疗效果进行体内监测。