Data Unit, Centre for Infectious Disease Research, Lusaka, Zambia.
Implementation Science Unit, Centre for Infectious Disease Research, Lusaka, Zambia.
J Med Internet Res. 2024 Sep 30;26:e54304. doi: 10.2196/54304.
This pilot study evaluates the effectiveness of mobile talk-time incentives in maintaining participation in a longitudinal mobile health (mHealth) data collection program among people living with HIV in Lusaka, Zambia. While mHealth tools, such as mobile phone surveys, provide vital health feedback, optimal incentive strategies to ensure long-term engagement remain limited. This study explores how different incentive levels affect response rates in multiple survey rounds, providing insights into effective methods for encouraging ongoing participation, especially in the context of Zambia's prepaid mobile system and multi-SIM usage, a common practice in sub-Saharan Africa.
This study aimed to assess the response rate success across multiple invitations to participate in a care experience survey using a mobile phone short codes and unstructured supplementary service data (USSD) model among individuals in an HIV care setting in the Lusaka, Zambia.
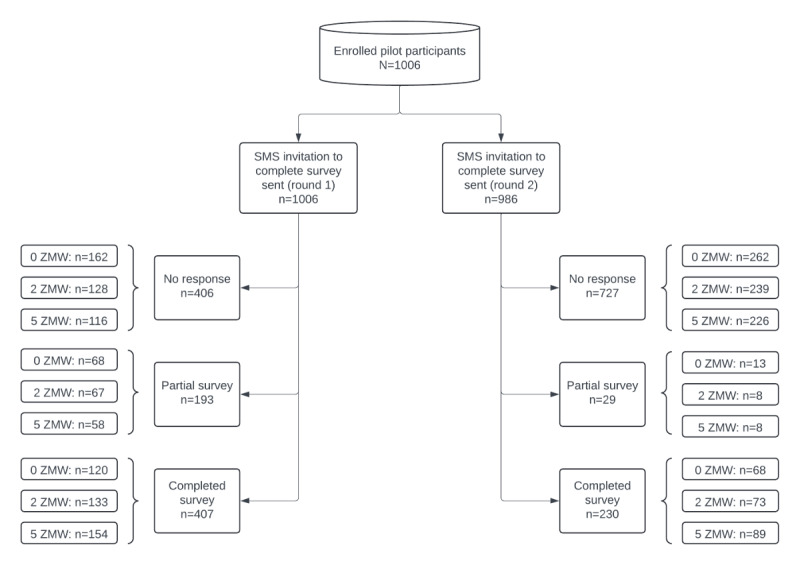
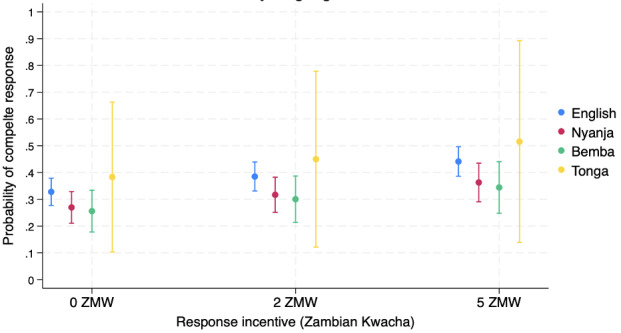
Participants were recruited from 2 study clinics-1 in a periurban setting and 1 in an urban setting. A total of 2 rounds of survey invitations were sent to study participants on a 3-month interval between November 1, 2018, and September 23, 2019. Overall, 3 incentive levels were randomly assigned by participant and survey round: (1) no incentive, (2) 2 Zambian Kwacha (ZMW; US $0.16), and (3) 5 ZMW (US $0.42). Survey response rates were analyzed using mixed-effects Poisson regression, adjusting for individual- and facility-level factors. Probability plots for survey completion were generated based on language, incentive level, and survey round. We projected the cost per additional response for different incentive levels.
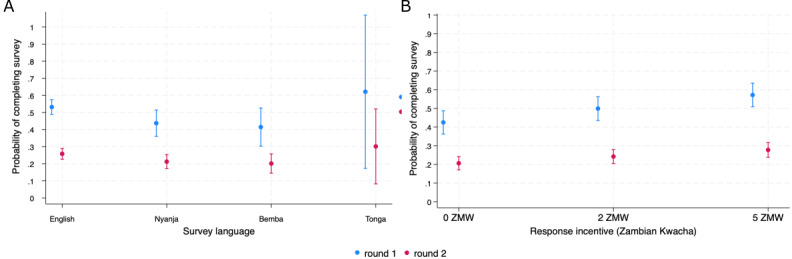
A total of 1006 participants were enrolled, with 72.3% (727/1006) from the urban HIV care facility and 62.4% (628/1006) requesting the survey in English. We sent a total of 1992 survey invitations for both rounds. Overall, survey completion across both surveys was 32.1% (637/1992), with significantly different survey completion between the first (40.5%, 95% CI 37.4-43.6%) and second (23.7%, 95% CI 21.1-26.4) invitations. Implementing a 5 ZMW (US $0.42) incentive significantly increased the adjusted prevalence ratio (aPR) for survey completion compared with those that received no incentive (aPR 1.35, 95% CI 1.11-1.63). The cost per additional response was highest at 5 ZMW, equivalent to US $0.42 (72.8 ZMW [US $5.82] per 1% increase in response).
We observed a sharp decline of almost 50% in survey completion success from the initial invitation to follow-up survey administered 3 months later. This substantial decrease suggests that longitudinal data collection potential for a care experience survey may be limited without additional sensitization and, potentially, added survey reminders. Implementing a moderate incentive increased response rates to our health care experience survey. Tailoring survey strategies to accommodate language preferences and providing moderate incentives can optimize response rates in Zambia.
Pan African Clinical Trial Registry PACTR202101847907585; https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=14613.
本试点研究评估了在赞比亚卢萨卡为艾滋病毒感染者提供的纵向移动健康(mHealth)数据收集项目中,使用移动通话时间激励措施来维持参与度的效果。虽然移动健康工具,如移动电话调查,提供了重要的健康反馈,但确保长期参与的最佳激励策略仍然有限。本研究探讨了不同激励水平如何影响多轮调查的回复率,为鼓励持续参与提供了有价值的见解,特别是在赞比亚的预付费移动系统和多 SIM 卡使用(撒哈拉以南非洲常见的做法)的背景下。
本研究旨在评估在赞比亚卢萨卡的 HIV 护理环境中,使用手机短码和非结构化补充服务数据(USSD)模型向参与者发送多轮参与护理体验调查邀请时的回复率。
参与者是从 2 个研究诊所招募的,一个位于城市周边地区,另一个位于城市地区。在 2018 年 11 月 1 日至 2019 年 9 月 23 日期间,每 3 个月发送两轮调查邀请。总共随机分配了 3 个激励水平给参与者和调查轮次:(1)无激励,(2)2 赞比亚克瓦查(ZMW;0.16 美元),(3)5 ZMW(0.42 美元)。使用混合效应泊松回归分析调查响应率,调整个体和设施水平因素。根据语言、激励水平和调查轮次生成调查完成的概率图。我们为不同的激励水平计算了额外响应的成本。
共纳入 1006 名参与者,其中 72.3%(727/1006)来自城市 HIV 护理机构,62.4%(628/1006)要求用英语进行调查。我们总共发送了两轮到 1992 次调查邀请。总的来说,两轮调查的完成率为 32.1%(637/1992),第一次(40.5%,95%CI 37.4-43.6%)和第二次(23.7%,95%CI 21.1-26.4%)邀请的调查完成率有显著差异。与没有激励的参与者相比,实施 5 ZMW(0.42 美元)激励显著增加了调查完成的调整患病率比(aPR)(aPR 1.35,95%CI 1.11-1.63)。额外响应的成本最高为 5 ZMW,相当于 0.42 美元(72.8 ZMW[5.82 美元],每增加 1%的响应)。
我们观察到,从初始邀请到 3 个月后进行的后续调查,调查完成成功率急剧下降了近 50%。这种大幅下降表明,如果没有额外的宣传和潜在的额外调查提醒,纵向数据收集的潜力可能会受到限制。实施适度激励措施可以提高我们的医疗保健体验调查的回复率。调整调查策略以适应语言偏好并提供适度的激励措施,可以优化赞比亚的回复率。
泛非临床试验注册中心 PACTR202101847907585;https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=14613。