Departamento de Salud Pública y Materno-infantil, Complutense University of Madrid, Faculty of Medicine, Madrid, Spain
Instituto de Investigacion Hospital 12 de Octubre (imas12), Madrid, Spain.
BMJ Open. 2024 Sep 30;14(9):e089628. doi: 10.1136/bmjopen-2024-089628.
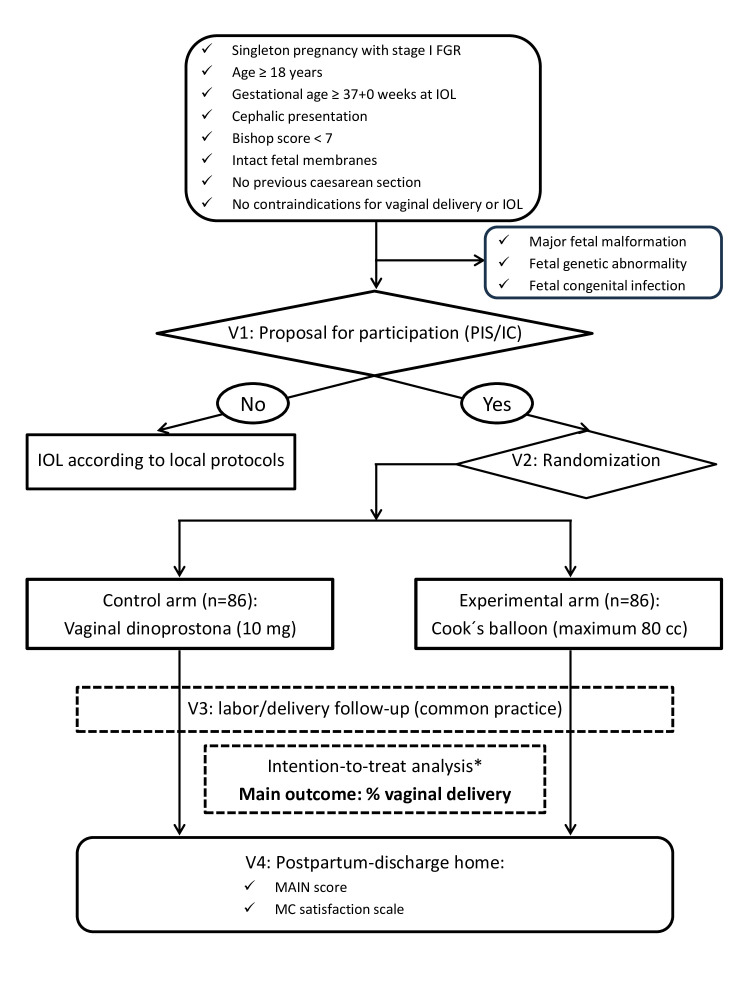
Fetal growth restriction (FGR) affects about 3%-5% of term pregnancies. If prenatally detected and anterograde umbilical artery flow is preserved (stage I), it is recommended to deliver at term (≥ 37+0 weeks). In the absence of contraindications, the vaginal route is preferred, and labour induction is usually required. It has been postulated that mechanical methods for cervical ripening may have an optimal profile for the induction of term FGR fetuses since they are associated with less uterine stimulation than the standard pharmacological methods, and therefore, could be better tolerated by fetuses with reduced placental reserve. This study aims to evaluate whether cervical ripening with a Cook's balloon for the induction of labour from 37+0 weeks of gestation in the stage I FGR manages to increase the rate of vaginal delivery compared with vaginal dinoprostone.
This will be an open-labelled, randomised, parallel-group clinical trial to be held in five Spanish maternities. Women aged ≥18 years with singleton pregnancies complicated with stage I FGR (defined as the presence of at least one of these two criteria: (1) estimated fetal weight (EFW) <3rd percentile; (2) EFW <10th percentile and at least one of the following: (2.1.) umbilical artery pulsatility index >95th percentile and presence of antegrade end-diastolic flow or (2.2.) Cerebroplacental ratio <5th percentile), gestational age dated by first-trimester ultrasound ≥37+0 weeks at the time of labour induction, cephalic presentation, unfavourable cervix (Bishop score <7), intact fetal membranes, no previous caesarean section and no maternal or fetal contraindications for vaginal delivery or labour induction will be 1:1 randomised by centre to labour induction with Cook's balloon (experimental arm) or dinoprostone (control arm). FGR cases with evidence of non-placental origin (major structural fetal malformations, chromosomal anomalies or congenital infection) will be excluded. The primary outcome is the achievement of a vaginal delivery and it will be assessed by comparing the rates of vaginal delivery in each group using the one-sided χ test at an alpha level of 0.025. The sample size has been estimated to observe an expected 84% of vaginal deliveries with Cook's balloon vs 62% with dinoprostone. Therefore, a total of 172 patients (86 per arm) are required (power of 90%, alpha level of 0.025, assuming a percentage of losses of 5%). The efficacy analysis will be performed in the intention-to-treat population. An interim analysis using a two-stage sequential design with the O'Brien-Fleming method will be applied.
The trial was registered in the European Union drug regulating authorities' clinical trials database (EUDRACT) (2021-001726-22) and received approval from the local Research Ethics Committee (21/728) and the Spanish Agency of Medicines and Medical Devices (AEMPS). AEMPS classified the study as a low-intervention trial. The study will be conducted in compliance with the principles of Good Clinical Practice. The study results will be disseminated through workshops and national/international conferences and published in peer-reviewed journals. In addition, they will be disclosed to patients and the public in understandable language through study newsletters and press releases to news and social media.
V.1.1, 18 May 2023.
EUDRACT 2021-001726-22 and NCT05774236.
胎儿生长受限(FGR)影响约 3%-5%的足月妊娠。如果产前发现并保持前向脐动脉血流(I 期),建议在足月(≥37+0 周)时分娩。如果没有禁忌症,首选阴道分娩,通常需要引产。有人假设,机械方法用于宫颈成熟可能对诱导足月 FGR 胎儿具有最佳的特征,因为它们与标准的药理学方法相比,对子宫的刺激较小,因此,对于胎盘储备减少的胎儿可能更容易耐受。本研究旨在评估在 I 期 FGR 中,从 37+0 周妊娠开始使用 Cook 气球进行宫颈成熟与阴道用普贝生相比,是否能提高阴道分娩率。
这将是一项在五个西班牙产科医院进行的开放标签、随机、平行组临床试验。年龄≥18 岁的单胎妊娠合并 I 期 FGR(定义为至少存在以下两个标准之一:(1)估计胎儿体重(EFW)<第 3 百分位;(2)EFW <第 10 百分位,且至少存在以下之一:(2.1)脐动脉搏动指数>第 95 百分位和存在前向舒张末期血流或(2.2)脑胎盘比值<第 5 百分位)、由孕早期超声确定的孕龄≥37+0 周、头位、宫颈不成熟(Bishop 评分<7)、胎膜完整、无既往剖宫产史且无阴道分娩或引产禁忌症的妇女将按中心 1:1 随机分为 Cook 气球(实验组)或普贝生(对照组)引产。有非胎盘起源证据的 FGR 病例(主要结构胎儿畸形、染色体异常或先天性感染)将被排除。主要结局是阴道分娩的实现,通过在单侧 α 水平为 0.025 时比较每组的阴道分娩率来评估,使用 χ 检验。根据 Cook 气球组 84%的阴道分娩率和普贝生组 62%的阴道分娩率,估计需要 172 名患者(每组 86 名)(90%的功效,α 水平为 0.025,假设失访率为 5%)。将在意向治疗人群中进行疗效分析。将应用 O'Brien-Fleming 方法的两阶段序贯设计进行中期分析。
该试验已在欧盟药品监管机构临床试验数据库(EUDRACT)(2021-001726-22)中注册,并获得当地伦理委员会(21/728)和西班牙药品和医疗器械管理局(AEMPS)的批准。AEMPS 将该研究归类为低干预试验。该研究将按照良好临床实践的原则进行。研究结果将通过研讨会和国家/国际会议进行传播,并发表在同行评议的期刊上。此外,将通过研究通讯和新闻稿以通俗易懂的语言向患者和公众公布,并通过新闻和社交媒体向公众公布。
V.1.1,2023 年 5 月 18 日。
EUDRACT 2021-001726-22 和 NCT05774236。