Pumas-AI, Inc, Dover, Delaware, USA.
Division of Clinical Pharmacology & Toxicology, The Hospital for Sick Children, Toronto, Ontario, Canada.
Clin Transl Sci. 2024 Oct;17(10):e70040. doi: 10.1111/cts.70040.
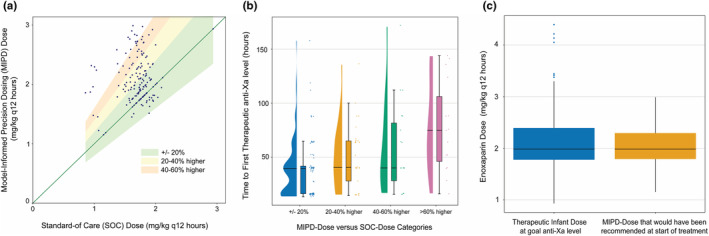
Traditional milligram per kilogram (mg/kg) dosing of enoxaparin in neonates frequently fails to achieve target anti-Xa levels promptly, necessitating repeated laboratory monitoring and dose adjustments. This study investigated whether a personalized dosing strategy based on predicted individual clearance and volume of distribution could improve outcomes, comparing standard-of-care (SOC) mg/kg dosing to pharmacokinetic (PK) model-informed precision dosing (MIPD). A retrospective analysis was conducted on hospitalized neonates treated with enoxaparin at less than 44 weeks postmenstrual age from 2019 to 2022. Data on demographics, drug dosing, PK model covariates, and clinical outcomes were extracted from electronic health records and analyzed using the Pumas-AI Lyv dosing tool. The primary focus was on comparing the initial SOC dose to the MIPD-recommended dose. The secondary outcome measured was the time required to achieve therapeutic anti-Xa levels. The study included 168 neonates with a median postnatal age of 15 days (range 1-149) and a median dosing weight of 3.1 kg (range: 0.82-5.2). MIPD-recommended initial doses were 20%-60% higher than SOC doses in 32% of the cases and over 60% higher in 11% of cases. Neonates who received SOC doses that were much lower than the MIPD recommendation showed the longest delays in reaching therapeutic anti-Xa levels. The results indicate that PK model-informed of enoxaparin dosing leads to higher initial dosages than SOC in neonates, potentially reducing the time to therapeutic anti-Xa levels. These findings are being utilized to define dosing limits for a prospective trial of MIPD in neonatal intensive care settings.
传统的新生儿依毫克/每公斤体重(mg/kg)给予依诺肝素,往往无法迅速达到目标抗-Xa 水平,需要反复进行实验室监测和剂量调整。本研究旨在探讨基于预测的个体清除率和分布容积的个体化给药策略是否可以改善结局,将标准治疗(SOC)mg/kg 剂量与基于药代动力学(PK)模型的精准给药(MIPD)进行比较。对 2019 年至 2022 年期间,胎龄不足 44 周的住院新生儿进行了回顾性分析,这些新生儿接受了依诺肝素治疗。从电子病历中提取人口统计学数据、药物剂量、PK 模型协变量和临床结局数据,并使用 Pumas-AI Lyv 给药工具进行分析。主要关注点是比较初始 SOC 剂量与 MIPD 推荐剂量。次要结局是达到治疗性抗-Xa 水平所需的时间。该研究纳入了 168 名新生儿,其平均出生后年龄为 15 天(范围 1-149),平均用药体重为 3.1kg(范围:0.82-5.2)。在 32%的病例中,MIPD 推荐的初始剂量比 SOC 剂量高 20%-60%,在 11%的病例中,初始剂量比 SOC 剂量高 60%以上。接受 SOC 剂量远低于 MIPD 建议剂量的新生儿,达到治疗性抗-Xa 水平的时间最长。结果表明,PK 模型指导的依诺肝素给药导致新生儿的初始剂量高于 SOC,可能缩短达到治疗性抗-Xa 水平的时间。这些发现正在用于定义前瞻性新生儿重症监护室 MIPD 试验的给药限制。