Lopez Christian J, Neil-Sztramko Sarah E, Tanyoas Mounir, Campbell Kristin L, Bender Jackie L, Strudwick Gillian, Langelier David M, Reiman Tony, Greenland Jonathan, Jones Jennifer M
Department of Supportive Care, Princess Margaret Cancer Centre, Toronto, Ontario, Canada.
Institute of Medical Science, University of Toronto, Toronto, Ontario, Canada.
Implement Sci Commun. 2024 Oct 1;5(1):108. doi: 10.1186/s43058-024-00650-4.
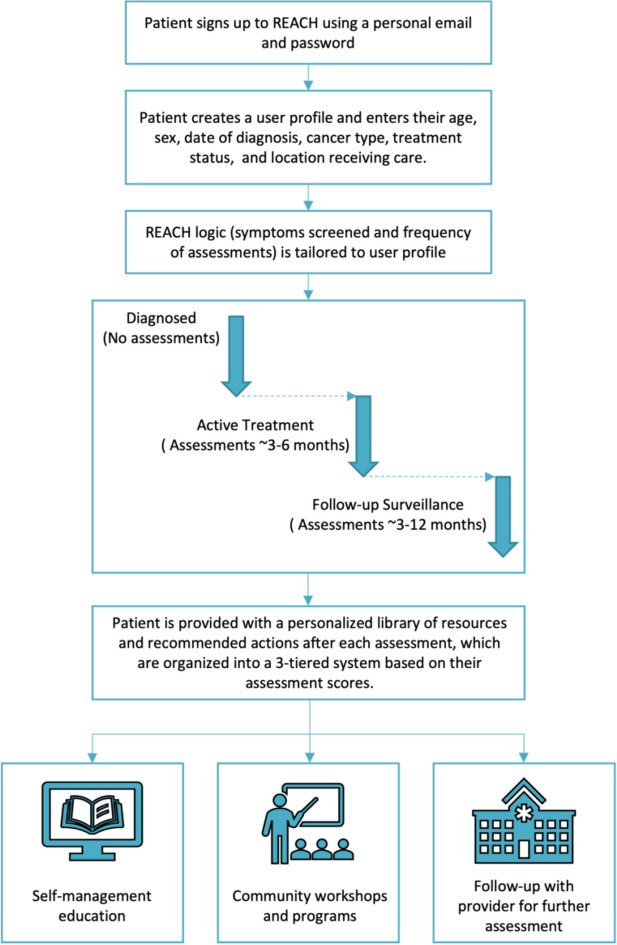
Electronic Prospective Surveillance Models (ePSMs) remotely monitor the rehabilitation needs of people with cancer via patient-reported outcomes at pre-defined time points during cancer care and deliver support, including links to self-management education and community programs, and recommendations for further clinical screening and rehabilitation referrals. Previous guidance on implementing ePSMs lacks sufficient detail on approaches to select implementation strategies for these systems. The purpose of this article is to describe how we developed an implementation plan for REACH, an ePSM system designed for breast, colorectal, lymphoma, and head and neck cancers.
Implementation Mapping guided the process of developing the implementation plan. We integrated findings from a scoping review and qualitative study our team conducted to identify determinants to implementation, implementation actors and actions, and relevant outcomes. Determinants were categorized using the Consolidated Framework for Implementation Research (CFIR), and the implementation outcomes taxonomy guided the identification of outcomes. Next, determinants were mapped to the Expert Recommendations for Implementing Change (ERIC) taxonomy of strategies using the CFIR-ERIC Matching Tool. The list of strategies produced was refined through discussion amongst our team and feedback from knowledge users considering each strategy's feasibility and importance rating via the Go-Zone plot, feasibility and applicability to the clinical contexts, and use among other ePSMs reported in our scoping review.
Of the 39 CFIR constructs, 22 were identified as relevant determinants. Clinic managers, information technology teams, and healthcare providers with key roles in patient education were identified as important actors. The CFIR-ERIC Matching Tool resulted in 50 strategies with Level 1 endorsement and 13 strategies with Level 2 endorsement. The final list of strategies included 1) purposefully re-examine the implementation, 2) tailor strategies, 3) change record systems, 4) conduct educational meetings, 5) distribute educational materials, 6) intervene with patients to enhance uptake and adherence, 7) centralize technical assistance, and 8) use advisory boards and workgroups.
We present a generalizable method that incorporates steps from Implementation Mapping, engages various knowledge users, and leverages implementation science frameworks to facilitate the development of an implementation strategy. An evaluation of implementation success using the implementation outcomes framework is underway.
电子前瞻性监测模型(ePSMs)通过在癌症治疗的预定义时间点收集患者报告的结果,远程监测癌症患者的康复需求,并提供支持,包括自我管理教育和社区项目的链接,以及进一步临床筛查和康复转诊的建议。以往关于实施ePSMs的指南在选择这些系统实施策略的方法上缺乏足够的细节。本文旨在描述我们如何为REACH(一个为乳腺癌、结直肠癌、淋巴瘤和头颈癌设计的ePSM系统)制定实施计划。
实施映射指导了实施计划的制定过程。我们整合了团队进行的范围审查和定性研究的结果,以确定实施的决定因素、实施者和行动以及相关结果。使用实施研究综合框架(CFIR)对决定因素进行分类,实施结果分类法指导结果的识别。接下来,使用CFIR-ERIC匹配工具将决定因素映射到实施变革专家建议(ERIC)策略分类法。通过团队讨论和知识使用者的反馈对生成的策略列表进行完善,知识使用者通过Go-Zone图考虑每个策略的可行性和重要性评级、对临床环境的可行性和适用性,以及我们范围审查中报告的其他ePSMs中的使用情况。
在39个CFIR构建体中,22个被确定为相关决定因素。在患者教育中起关键作用的诊所经理、信息技术团队和医疗保健提供者被确定为重要实施者。CFIR-ERIC匹配工具产生了50个获得一级认可的策略和13个获得二级认可的策略。最终的策略列表包括:1)有目的地重新审视实施情况;2)调整策略;3)更改记录系统;4)召开教育会议;5)分发教育材料;6)对患者进行干预以提高接受度和依从性;7)集中技术援助;8)使用咨询委员会和工作组。
我们提出了一种可推广的方法,该方法纳入了实施映射的步骤,吸引了各种知识使用者,并利用实施科学框架来促进实施策略的制定。目前正在使用实施结果框架对实施成功情况进行评估。