Dubberke Erik R, Li Qinghua, Obi Engels N, Turzhitsky Vladimir, Siddiqui Fakhar, Nathanson Brian H
Washington University School of Medicine, Saint Louis, Missouri, USA.
Merck & Co., Inc., Rahway, New Jersey, USA.
Open Forum Infect Dis. 2024 Sep 30;11(10):ofae524. doi: 10.1093/ofid/ofae524. eCollection 2024 Oct.
The 2021 update to the Infectious Diseases Society of America infection (CDI) guidelines recommended fidaxomicin as the preferred treatment over vancomycin for patients with initial and recurrent CDI. Few studies have examined how treatment patterns and clinical outcomes of hospitalized CDI patients changed after the postguideline update or contemporary real-world outcomes of fidaxomicin vs vancomycin.
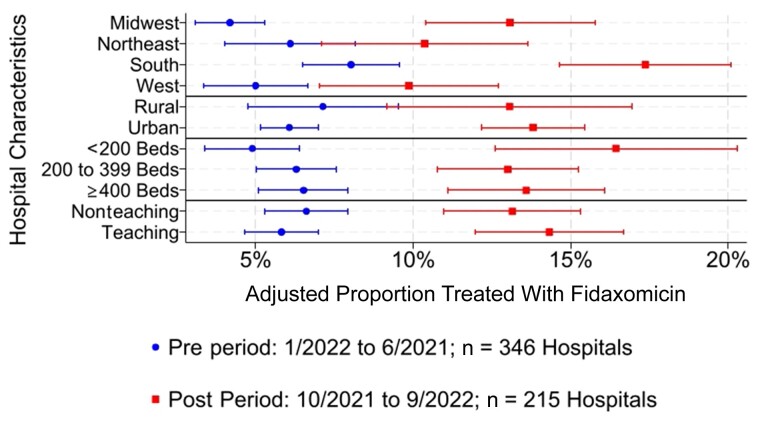
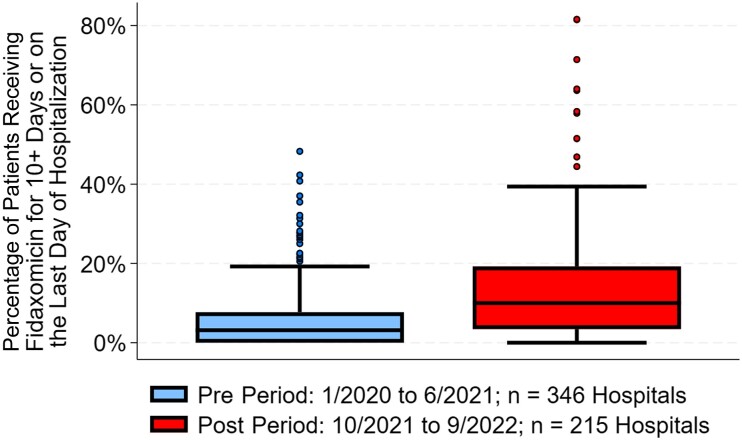
This retrospective, observational study used the PINC AI Healthcare Database on adult patients who received CDI treatment between 1/2020 and 6/2021 (pre period) and between 10/2021 and 9/2022 (post period). We examined treatment patterns of fidaxomicin, vancomycin, and metronidazole, as well as clinical and health care resource use outcomes of patients treated exclusively with fidaxomicin vs vancomycin, using nearest-neighbor propensity matching and hierarchical regression methods. As a sensitivity analysis, we repeated the fidaxomicin vs vancomycin comparisons among patients with recurrent and nonrecurrent index infections.
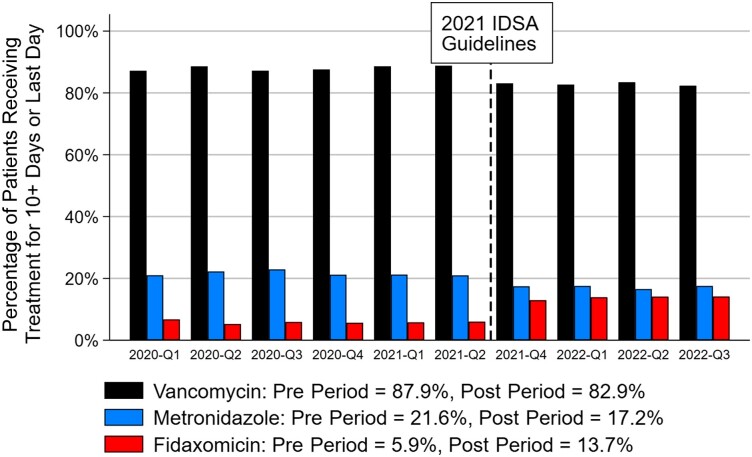
A total of 45 049 patients with CDI from 779 US hospitals met initial inclusion criteria. Comparing the pre vs post periods, the proportion of patients treated with fidaxomicin increased from 5.9% to 13.7% ( < .001), vancomycin use decreased from 87.9% to 82.9% ( < .001), and metronidazole use decreased from 21.6% to 17.2% ( < .001). When comparing fidaxomicin vs vancomycin in the post period, fidaxomicin was associated with lower CDI recurrence (6.1% vs 10.2%; < .001) and higher sustained clinical response (91.7% vs 87.8%; < .001). Ninety-day postdischarge costs were not significantly different between groups. A sensitivity analyses showed similar findings.
Since the 2021 guideline update, fidaxomicin use has increased significantly but could be further utilized given its association with better clinical outcomes and no increase in postdischarge costs.
美国传染病学会2021年更新的艰难梭菌感染(CDI)指南推荐,对于初发和复发性CDI患者,非达霉素是比万古霉素更优选的治疗药物。很少有研究探讨在指南更新后住院CDI患者的治疗模式和临床结局如何变化,以及非达霉素与万古霉素的当代真实世界结局。
这项回顾性观察研究使用了PINC AI医疗数据库,纳入了在2020年1月至2021年6月(前期)以及2021年10月至2022年9月(后期)接受CDI治疗的成年患者。我们使用最近邻倾向匹配和分层回归方法,研究了非达霉素、万古霉素和甲硝唑的治疗模式,以及仅接受非达霉素与万古霉素治疗的患者的临床和医疗资源使用结局。作为敏感性分析,我们在复发性和非复发性索引感染患者中重复了非达霉素与万古霉素的比较。
来自779家美国医院的45049例CDI患者符合初始纳入标准。比较前期和后期,接受非达霉素治疗的患者比例从5.9%增至13.7%(P<0.001),万古霉素的使用从87.9%降至82.9%(P<0.001),甲硝唑的使用从21.6%降至17.2%(P<0.001)。在后期比较非达霉素与万古霉素时,非达霉素与较低的CDI复发率相关(6.1%对10.2%;P<0.001),且持续临床缓解率更高(91.7%对87.8%;P<0.001)。两组出院后90天的费用无显著差异。敏感性分析显示了类似的结果。
自2021年指南更新以来,非达霉素的使用显著增加,但鉴于其与更好的临床结局相关且出院后费用未增加,其使用仍可进一步提高。