Khazali S, Bachi A, Mondelli B, Fleischer K, Adamczyk M, Delanerolle G, Shi J Q, Yang X, Nisar P, Bearn P
Facts Views Vis Obgyn. 2024 Sep;16(3):325-336. doi: 10.52054/FVVO.16.3.030.
Endometriosis surgery outcomes have been widely studied, yet heterogeneity in terminology and techniques persist.
This study focuses on the perioperative outcomes of a single surgeon using the same structured approach (SOSURE: Survey & Sigmoid mobilisation, Ovarian mobilisation, Suspension of uterus and ovaries, Ureterolysis, Rectovaginal and pararectal space development, Excision of all visible disease) and adheres to the recent standardised terminology proposed by international gynaecological and endometriosis societies.
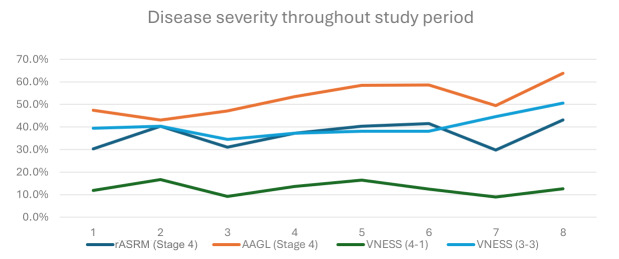
A quality improvement study was conducted retrospectively from January 2015 to January 2023. Data collection involved two databases: the National British Society for Gynaecological Endoscopy (BSGE) database and a more comprehensive locally kept database. The methodology also integrated four endometriosis staging systems.
Intra-operative and post-operative complication rates.
Between 2015 and 2023, 1047 women underwent 1116 endometriosis procedures in various UK hospitals with S.K. as primary surgeon. Exclusions totalled 20 due to missing records and specific surgical criteria. The rate of major post-operative complications (Clavien-Dindo grade 3a and 3b) was 1.5% and minor post-operative complications (Clavien-Dindo grade 1 and 2) were seen in 13.8%. No Clavien-Dindo grade 4 or 5 complications were noted.
Our study has shown a low complication rate in endometriosis surgery, despite increasing complexity of surgical cases. This is likely attributed to the surgeon's learning curve, high surgical volume and adherence to a structured approach.
WHAT'S NEW?: Our study demonstrates the learning curve of a surgeon over the course of 8 years. This series involved more than 1000 patients and to our knowledge, is the first to report the complexity of the casemix using four different endometriosis staging systems.
子宫内膜异位症手术的结果已得到广泛研究,但术语和技术的异质性仍然存在。
本研究聚焦于单一外科医生采用相同结构化方法(SOSURE:探查与乙状结肠游离、卵巢游离、子宫和卵巢悬吊、输尿管松解、直肠阴道和直肠旁间隙拓展、切除所有可见病灶)的围手术期结果,并遵循国际妇科和子宫内膜异位症协会最近提出的标准化术语。
2015年1月至2023年1月进行了一项回顾性质量改进研究。数据收集涉及两个数据库:英国国家妇科内镜学会(BSGE)数据库和一个更全面的本地保存数据库。该方法还整合了四种子宫内膜异位症分期系统。
术中及术后并发症发生率。
2015年至2023年期间,在英国各医院,1047名女性接受了1116例子宫内膜异位症手术,主刀医生为S.K.。因记录缺失和特定手术标准,共排除20例。术后严重并发症(Clavien-Dindo 3a和3b级)发生率为1.5%,术后轻微并发症(Clavien-Dindo 1和2级)发生率为13.8%。未发现Clavien-Dindo 4级或5级并发症。
我们的研究表明,尽管手术病例的复杂性增加,但子宫内膜异位症手术的并发症发生率较低。这可能归因于外科医生的学习曲线、高手术量以及对结构化方法的遵循。
我们的研究展示了一名外科医生在8年期间的学习曲线。该系列涉及1000多名患者,据我们所知,这是首次使用四种不同的子宫内膜异位症分期系统报告病例组合的复杂性。