Nevin Amy N, Atresh Sridhar S, Vivanti Angela, Ward Leigh C, Hickman Ingrid J
Department of Nutrition and Dietetics, Princess Alexandra Hospital, Brisbane, QLD, Australia.
The Hopkins Centre, School of Health Sciences and Social Work, Griffith University, Brisbane, QLD, Australia.
Spinal Cord Ser Cases. 2024 Oct 2;10(1):70. doi: 10.1038/s41394-024-00682-x.
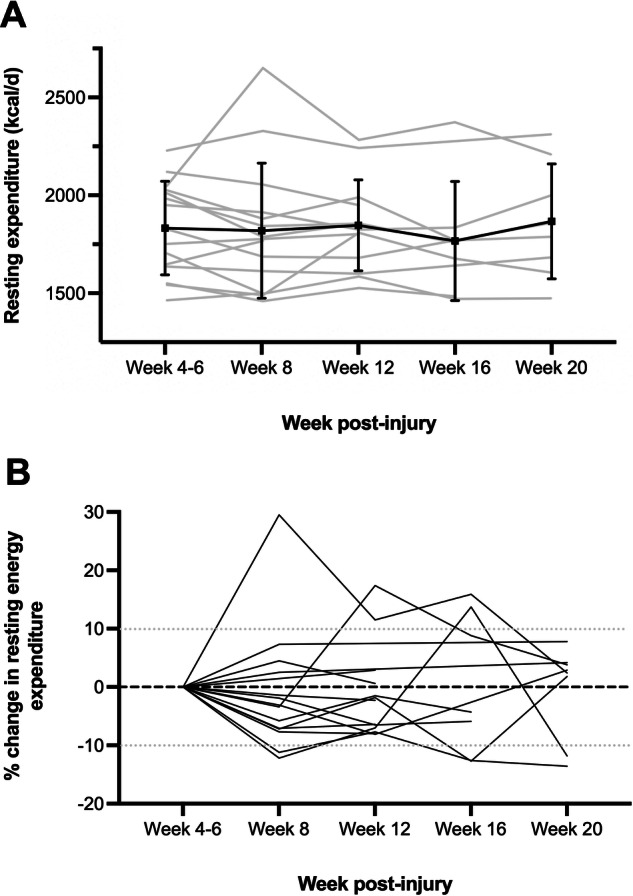
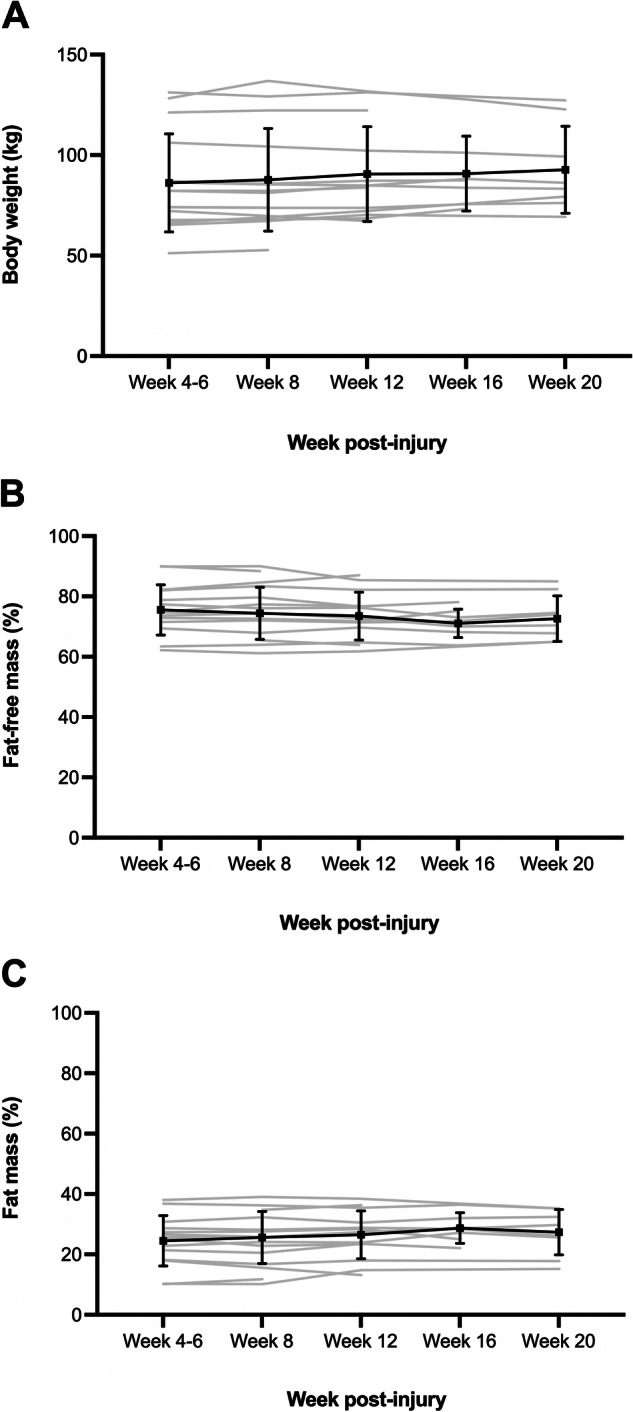
Longitudinal observational study. Measurements were undertaken between weeks 4-6 post-spinal cord injury (SCI), repeated at week 8 and every 4 weeks thereafter until week 20 or rehabilitation discharge, whichever occurred first.
Observe variation in measured resting energy expenditure (REE) and body composition in males undergoing SCI rehabilitation, compare REE with SCI-specific prediction equations incorporating fat-free mass (FFM), and explore the prevalence of clinical factors that may influence individual REE.
Spinal Injuries Unit, Brisbane, Queensland, Australia.
Indirect calorimetry was used to measure REE and bioimpedance spectroscopy to assess body composition. Four SCI-specific FFM-based REE and basal metabolic rate (BMR) prediction equations were compared to measured REE. A clinically significant change in REE was defined as +/- 10% difference from the week 4-6 measurement. Clinical factors that may affect REE variations were collected including infection, pressure injuries, autonomic dysreflexia, spasticity, and medications.
Fifteen people participated (mean age 35 ± 13 years, 67% paraplegic). There was no statistically significant change in mean REE, weight, or body composition, and the Chun and Nightingale BMR prediction equations performed best (r > 0.8 at all time points). One-third of participants had >10% change in REE on 11 occasions, with clinical factors not consistently associated with the observed changes.
During SCI rehabilitation, mean REE, weight, and body composition remain unchanged, and FFM-based BMR prediction equations may be an acceptable alternative to indirect calorimetry. Future research designs should avoid single indirect calorimetry measures as snapshot data may not represent typical REE in this population.
纵向观察性研究。在脊髓损伤(SCI)后第4至6周进行测量,第8周重复测量,此后每4周测量一次,直至第20周或康复出院,以先到者为准。
观察接受SCI康复治疗的男性静息能量消耗(REE)和身体成分的变化,将REE与纳入去脂体重(FFM)的SCI特异性预测方程进行比较,并探讨可能影响个体REE的临床因素的患病率。
澳大利亚昆士兰州布里斯班脊髓损伤科。
采用间接测热法测量REE,生物电阻抗光谱法评估身体成分。将四个基于SCI特异性FFM的REE和基础代谢率(BMR)预测方程与测量的REE进行比较。REE的临床显著变化定义为与第4至6周测量值相差±10%。收集可能影响REE变化的临床因素,包括感染、压疮、自主神经反射异常、痉挛和药物。
15人参与研究(平均年龄35±13岁,67%为截瘫患者)。平均REE、体重或身体成分无统计学显著变化,Chun和Nightingale BMR预测方程表现最佳(在所有时间点r>0.8)。三分之一的参与者在11次测量中有>10%的REE变化,临床因素与观察到的变化无一致关联。
在SCI康复期间,平均REE、体重和身体成分保持不变,基于FFM的BMR预测方程可能是间接测热法的可接受替代方法。未来的研究设计应避免单次间接测热法测量,因为快照数据可能无法代表该人群的典型REE。