McLaren John R, Nascimento Fábio A, Chakranarayan Joshua, Olandoski Marcia, Veerapaneni Poornachand, Gavvala Jay R
From the Department of Neurology (J.R.M.), Boston Children's Hospital, MA; Department of Neurology (F.A.N.), Washington University School of Medicine, St. Louis, MO; Department of Adult Neurology (J.C., P.V.), Baylor College of Medicine, Houston, TX; School of Medicine (M.O.), Pontifícia Universidade Católica do Paraná, Curitiba, Brazil; and Department of Neurology (J.R.G.), McGovern Medical School, Houston, TX.
Neurol Educ. 2024 Mar 13;3(1):e200120. doi: 10.1212/NE9.0000000000200120. eCollection 2024 Mar.
Given the inherent risks of seizure provocation in the epilepsy monitoring unit (EMU), both miscommunication and incomplete training about the importance of when and why certain measures are taken can cause critical gaps in care for patients in an especially vulnerable state. To provide a framework that would help minimize these potential pitfalls, our objectives were 2-fold: (1) identify deficits in EMU safety and assessment using a checklist of predetermined items, including key measures essential to the care of EMU patients and (2) develop a simulation training program to address these deficits with education for staff on optimal practices.
After creation of an EMU safety checklist, authors retrospectively reviewed video from 12 consecutive patients (time zero; T0) admitted to the Baylor St. Luke's EMU to assess checklist compliance and seizure response times (both electrographic and clinical). EMU staff were then trained in small teams with the help of a simulation program developed using a high-fidelity manikin. After training was complete, EMU practices and response times were reassessed in short-term (T1) and long-term (T2) follow-up intervals.
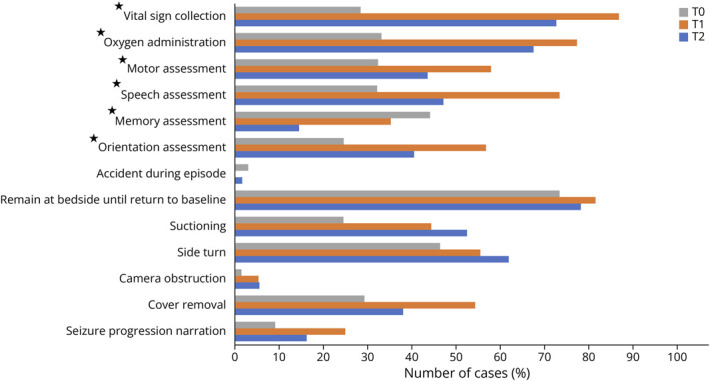
When all 3 groups were compared, significant behavioral improvements (Kirkpatrick level 3) were seen in several critical evaluation and safety measures. Statistically significant improvements from T0 to T1 ( < 0.05) were seen in orientation assessment, speech assessment, motor assessment, oxygen administration, and vital sign collection. Score improvement persisted at T2 but showed a relative decline over time in 11 of 14 measures.
Education of staff in the EMU is paramount to ensure appropriate assessment of the seizure semiology and patient safety measures. Implementation of a novel simulation-based education platform demonstrated wide-ranging improvements in staff performance of safety and testing measures. Stratification between short-term and long-term assessment periods shows that while many categories showed overall improvement, regular training may be needed to sustain improvements in assessment and patient safety. Multicenter longitudinal studies assessing the efficacy of this or similar interventions should be performed to identify best patient practices.
鉴于癫痫监测单元(EMU)中诱发癫痫存在固有风险,关于何时以及为何采取某些措施的重要性方面的沟通不畅和培训不完整,可能会在护理处于特别脆弱状态的患者时造成关键的护理缺口。为了提供一个有助于将这些潜在陷阱降至最低的框架,我们的目标有两个:(1)使用预先确定项目的清单,包括对EMU患者护理至关重要的关键措施,识别EMU安全和评估方面的缺陷;(2)制定一个模拟培训计划,通过对工作人员进行最佳实践教育来解决这些缺陷。
在创建EMU安全清单后,作者回顾性分析了连续收治到贝勒圣卢克EMU的12例患者(时间零点;T0)的视频,以评估清单的依从性和癫痫发作反应时间(包括脑电图和临床发作反应时间)。然后,在使用高仿真人体模型开发的模拟程序的帮助下,对EMU工作人员进行小组培训。培训完成后,在短期(T1)和长期(T2)随访期间重新评估EMU的实践和反应时间。
当对所有三组进行比较时,在一些关键评估和安全措施方面观察到显著的行为改善(柯克帕特里克3级)。从T0到T1,在定向评估、言语评估、运动评估、氧气供应和生命体征采集方面有统计学意义的改善(<0.05)。在T2时得分改善持续存在,但在14项措施中的11项中,随着时间推移显示出相对下降。
对EMU工作人员进行教育对于确保对癫痫发作症状学和患者安全措施进行适当评估至关重要。实施一个基于模拟的新型教育平台在工作人员的安全和测试措施表现方面显示出广泛的改善。短期和长期评估期之间的分层表明,虽然许多类别总体上有所改善,但可能需要定期培训以维持评估和患者安全方面的改善。应进行多中心纵向研究以评估此干预措施或类似干预措施的疗效,以确定最佳的患者护理实践。