Division of Hematology/Oncology, Department of Medicine, Larner College of Medicine at The University of Vermont, Burlington, VT.
Division of Clinical Pathology, Department of Pathology and Laboratory Medicine, Larner College of Medicine at The University of Vermont, Burlington, VT.
Blood Adv. 2024 Nov 26;8(22):5896-5905. doi: 10.1182/bloodadvances.2024013882.
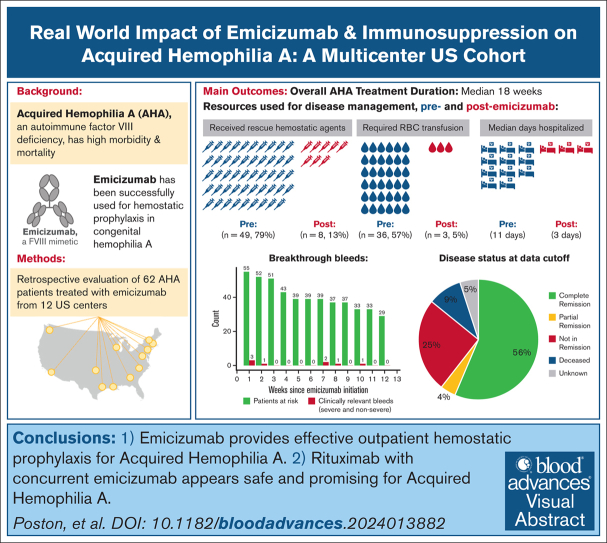
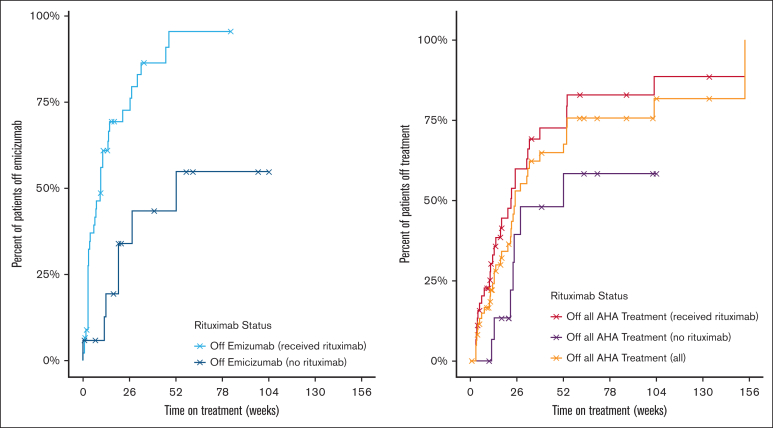
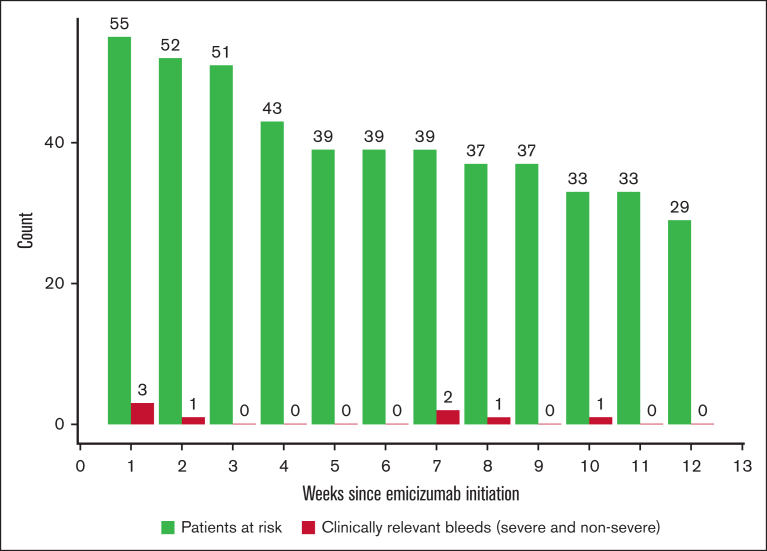
Acquired hemophilia A (AHA) is an autoimmune bleeding disorder that is caused by factor VIII (FVIII) autoantibodies with high morbidity and mortality due to bleeding and complications from immunosuppression (IST). To address the real-world implications of the FVIII mimetic antibody, emicizumab, and the role of IST, we retrospectively collected de-identified data on 62 patients with AHA who were treated off-label with emicizumab for a median of 10 weeks at 12 US-based hemophilia treatment centers. Most patients (95.2%) had acute bleeding at diagnosis, and 62.9% had partial or no control of bleeds despite the use of hemostatic agents at the time emicizumab was started. The main reason for initiating emicizumab was outpatient bleeding prophylaxis. After initiation of emicizumab, 87.1% had no additional bleeds. There were 6 breakthrough bleeds (2 spontaneous) in 5 patients and no fatal bleeding events during maintenance emicizumab treatment. The mean breakthrough bleed rate per patient-week was 0.02 (95% confidence interval, 0.0-0.03) during the first 12 weeks of emicizumab for the 55 patients with at least 12 weeks of follow-up. Of these patients, 92.7% received IST and 74.5% were prescribed rituximab-based regimens. Complete resolution of inhibitor and normalization of FVIII levels occurred in 56% overall and in 63% of the patients treated with rituximab. Overall, the median time to discontinuation of emicizumab and IST was 18 weeks. Two patients had thrombotic events while on emicizumab, but no adverse events were attributed to emicizumab and there were no infections attributed to IST. Emicizumab provides effective outpatient bleeding prophylaxis for AHA, and concurrent IST may further mitigate bleeding.
获得性血友病 A (AHA) 是一种由因子 VIII (FVIII) 自身抗体引起的自身免疫性出血性疾病,由于出血和免疫抑制 (IST) 相关并发症,其发病率和死亡率均较高。为了了解 FVIII 模拟抗体emicizumab 及 IST 的实际应用,我们回顾性收集了在 12 家美国血友病治疗中心,62 例 AHA 患者接受emicizumab 治疗的无标签数据。大多数患者(95.2%)在诊断时即有急性出血,62.9%的患者尽管在开始使用 emicizumab 时已使用止血药物,但仍存在部分或无出血控制。启动 emicizumab 的主要原因是门诊出血预防。启动 emicizumab 后,87.1%的患者无额外出血。5 例患者中有 6 例出现突破性出血(2 例自发性),在维持 emicizumab 治疗期间无致命性出血事件。在 55 例至少有 12 周随访的患者中,在 emicizumab 的前 12 周内,每位患者每周的突破性出血率平均为 0.02(95%置信区间,0.0-0.03)。这些患者中,92.7%接受 IST,74.5%接受基于利妥昔单抗的方案。总体上,抑制剂完全缓解且 FVIII 水平正常化的发生率为 56%,接受利妥昔单抗治疗的患者中为 63%。总体而言,停止使用 emicizumab 和 IST 的中位时间为 18 周。2 例患者在使用 emicizumab 时发生血栓事件,但无不良事件归因于 emicizumab,也无 IST 相关感染。Emicizumab 可为 AHA 提供有效的门诊出血预防,同时进行 IST 可能进一步减少出血。