Department of Internal Medicine and Hematology, Semmelweis University, Budapest, Hungary.
Department of Hematology and Stem Cell Transplantation, South-Pest Central Hospital, National Institute of Hematology and Infectious Disease, St. László Campus, Budapest, Hungary.
Blood. 2022 Nov 3;140(18):1983-1992. doi: 10.1182/blood.2022016873.
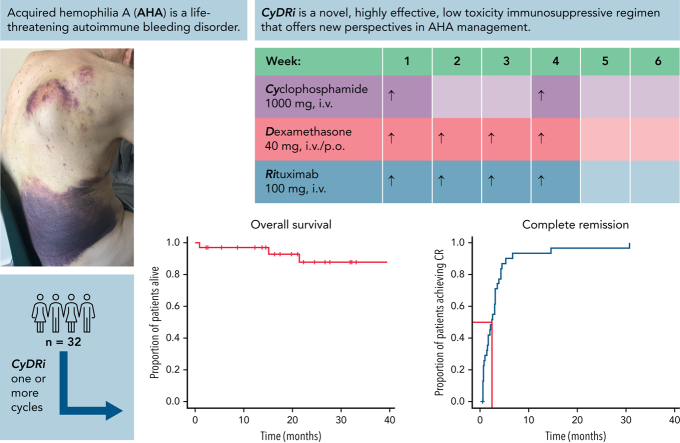
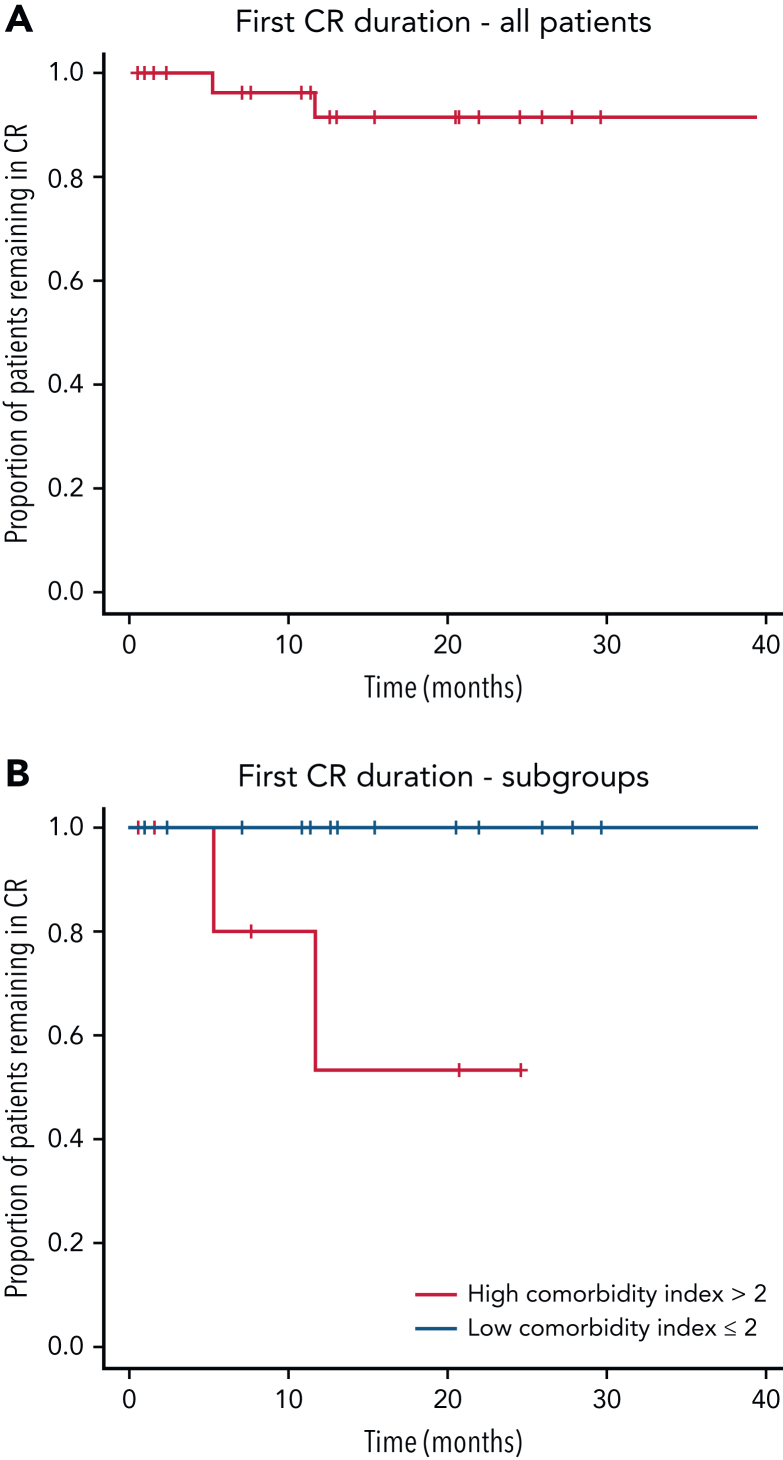
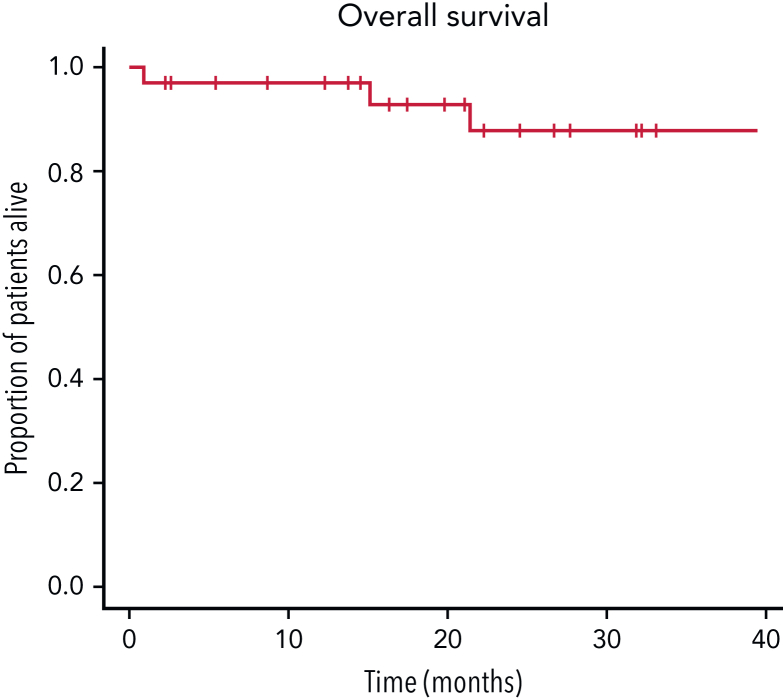
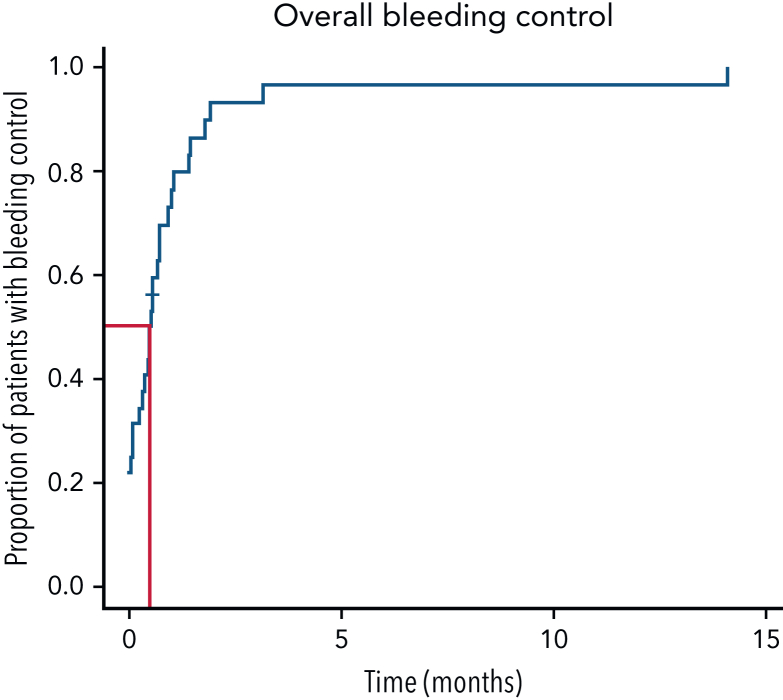
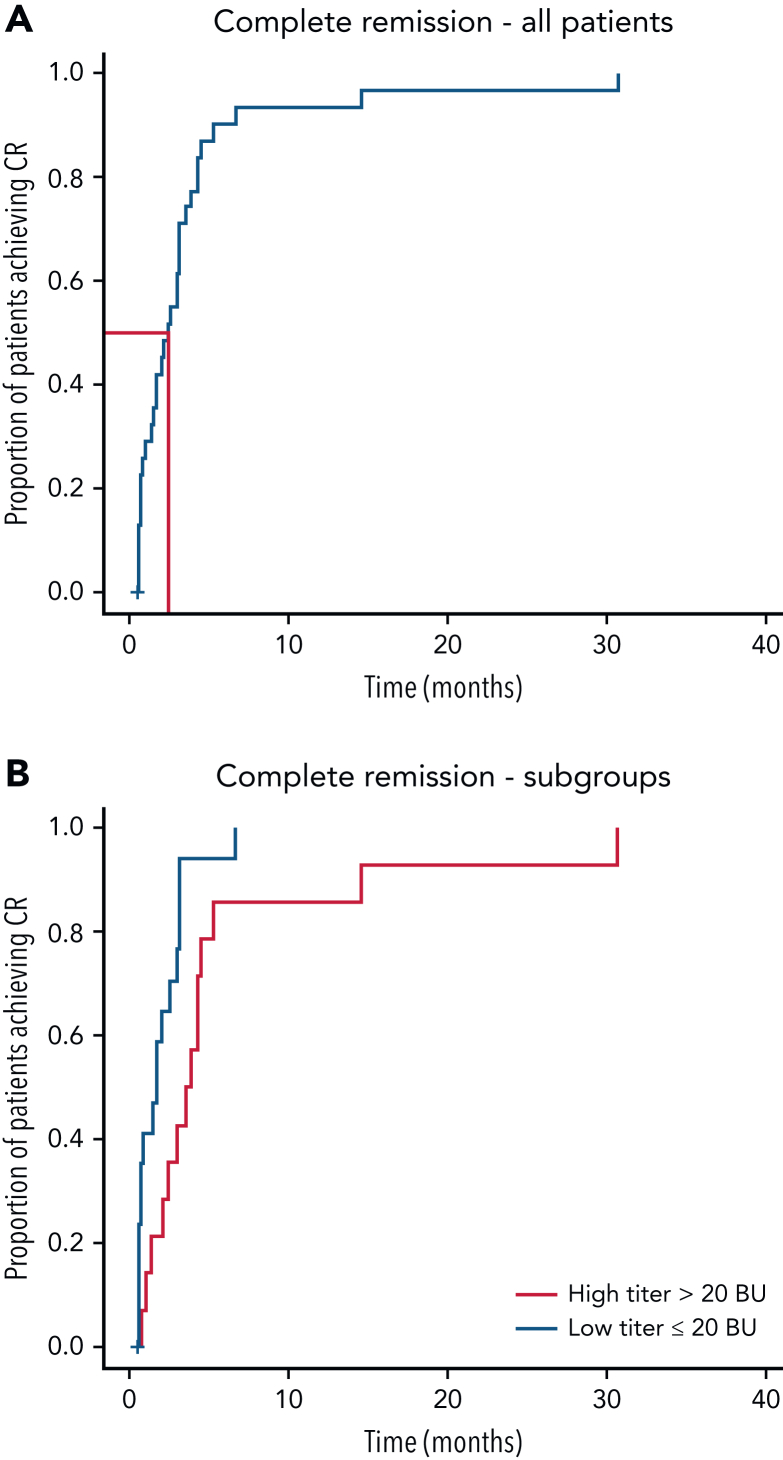
Acquired hemophilia A (AHA) is a rare severe autoimmune bleeding disorder with significant morbidity and mortality. Although critical for disease control, there is no consensus for the best immunosuppressive regimen. Most authors use steroids first line, followed by other agents for steroid failures. Upfront combined regimens offer the advantage of reduced steroid exposure and toxicity as well as increased efficacy. We retrospectively analyzed data from 32 patients with AHA treated on an identical such institutional protocol: cyclophosphamide 1000 mg on days 1 and 22, dexamethasone 40 mg on days 1, 8, 15, and 22, and rituximab 100 mg on days 1, 8, 15, and 22 (the regimen was termed CyDRi). All patients received at least 1 cycle of CyDRi. If necessary, CyDRi was repeated until remission, no sooner than day 43 of the previous cycle. Bleeding control was rapidly achieved. The median time for bleeding control was 15.5 days (range, 0-429 days; interquartile range, 2.5-29.5 days). Thirty-one (96.8%) of 32 patients achieved durable complete remission (CR); 29 (90.6%) of 32 patients were alive at last follow-up, all of them in CR. The median time to reach first CR was 77 days (range, 19-939 days; interquartile range, 31-115 days). Toxicity and side effects were acceptable and milder than those of commonly used, prolonged steroid therapies. In conclusion, the CyDRi regimen produced markedly higher CR rates and overall survival than currently used sequential regimens. Taken together, CyDRi proved to be an attractive option for the immunosuppression of elderly patients with AHA.
获得性血友病 A(AHA)是一种罕见的严重自身免疫性出血性疾病,具有显著的发病率和死亡率。虽然对于疾病控制至关重要,但对于最佳免疫抑制方案尚无共识。大多数作者首先使用类固醇,然后在类固醇治疗失败时使用其他药物。预先使用联合方案具有减少类固醇暴露和毒性以及提高疗效的优势。我们回顾性分析了 32 名接受相同机构方案治疗的 AHA 患者的数据:环磷酰胺 1000mg 于第 1 天和第 22 天,地塞米松 40mg 于第 1 天、第 8 天、第 15 天和第 22 天,利妥昔单抗 100mg 于第 1 天、第 8 天、第 15 天和第 22 天(该方案称为 CyDRi)。所有患者均接受至少 1 个周期的 CyDRi。如果需要,在第 43 天之前,直到缓解,且不早于前一个周期的第 43 天,重复使用 CyDRi。出血很快得到控制。出血控制的中位时间为 15.5 天(范围 0-429 天;四分位距 2.5-29.5 天)。32 例患者中有 31 例(96.8%)获得持久完全缓解(CR);32 例患者中有 29 例(90.6%)在最后一次随访时存活,且均处于 CR 状态。达到首次 CR 的中位时间为 77 天(范围 19-939 天;四分位距 31-115 天)。毒性和副作用是可以接受的,且比常用的、长期类固醇治疗的副作用更轻。总之,CyDRi 方案比目前使用的序贯方案产生了更高的 CR 率和总生存率。总的来说,CyDRi 被证明是治疗老年 AHA 患者的一种有吸引力的免疫抑制选择。