Togna Pabo Willy Le Roi, Kengni Ngueko Aurelie Minelle, Nka Alex Durand, Santoro Maria Mercedes, Bouba Yagai, Chenwi Collins Ambe, Ngoufack Jagni Semengue Ezéchiel, Takou Désiré, Teto Georges, Dambaya Beatrice, Nyasa Raymond Babila, Tommo Tchouaket Michel Carlos, Beloumou Grace Angong, Djupsa Ndjeyep Sandrine Claire, Ka'e Aude Christelle, Tekoh Tatiana Anim Keng, Ayuk Ngwese Derrick Tambe, Etame Naomi-Karell, Mundo Rachel Audrey Nayang, Kamgaing Rachel Simo, Sosso Samuel Martin, Ndip Roland Ndip, Colizzi Vittorio, Cecchereni-Silberstein Francesca, Ndjolo Alexis, Fokam Joseph
Chantal BIYA International Reference Centre for Research on HIV/AIDS Prevention and Management (CIRCB), Yaoundé, Cameroon.
Faculty of Science, University of Buea, Buea, Cameroon.
Front Med (Lausanne). 2024 Sep 20;11:1457501. doi: 10.3389/fmed.2024.1457501. eCollection 2024.
The elevated rate of AIDS-related mortality in Sub-Saharan Africa among adolescents living with HIV (ALHIV) is influenced by various factors, notably immunosuppression, within a framework of limited therapeutic alternatives. We aimed to enhance the management of pediatric HIV by assessing the immune response and associated factors in perinatally-infected ALHIV on antiretroviral therapy (ART) in Cameroon.
A cohort study was conducted from 2018-2020 among 271 ART-experienced ALHIV in Cameroon. Sociodemographic data, immunological (CD4), and virological (plasma viral load, PVL) responses were measured at enrolment (T0), 6-months (T1), and 12-months (T2) using PIMA CD4 (Abbott/Pantech (Pty) Ltd) and Abbott Applied Biosystem platform (Real-Time PCR m2000RT) respectively. Immunological failure (IF) was defined as absolute CD4 < 250 cells/mm, and Virological failure (VF) as PVL ≥ 1,000 copies/ml. A linear mixed-effects model with R version 4.4.1 was used to estimate both fixed and random effects, with significance set at < 0.05.
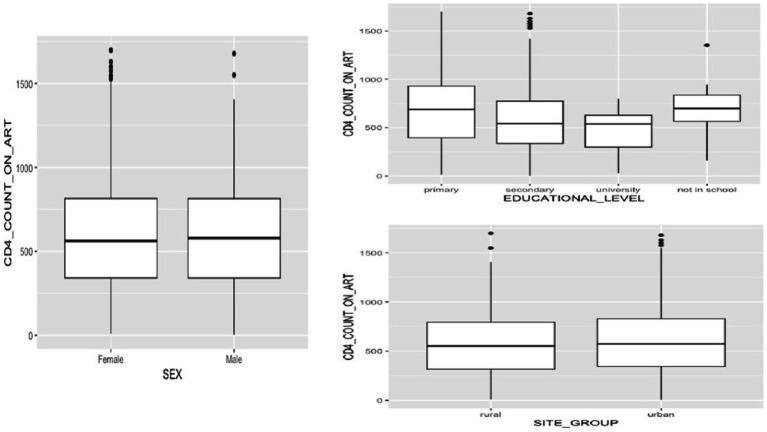
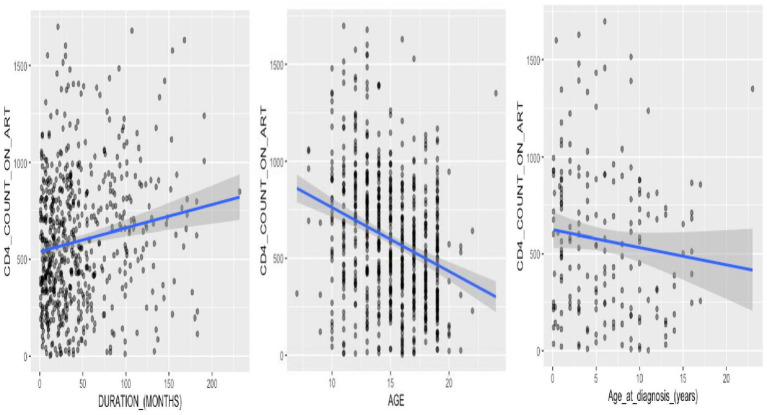
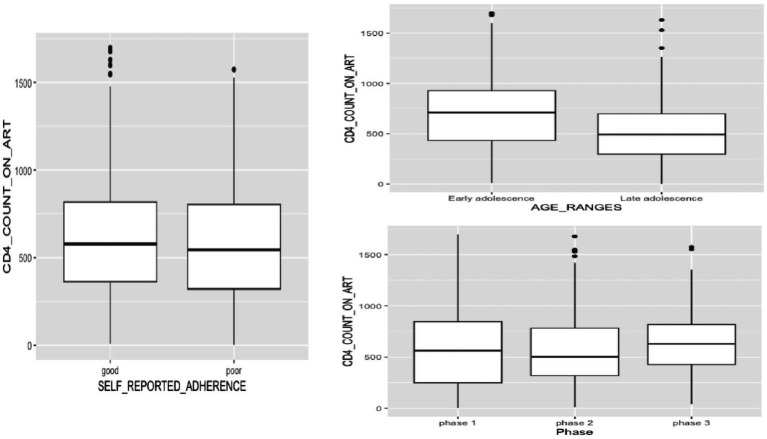
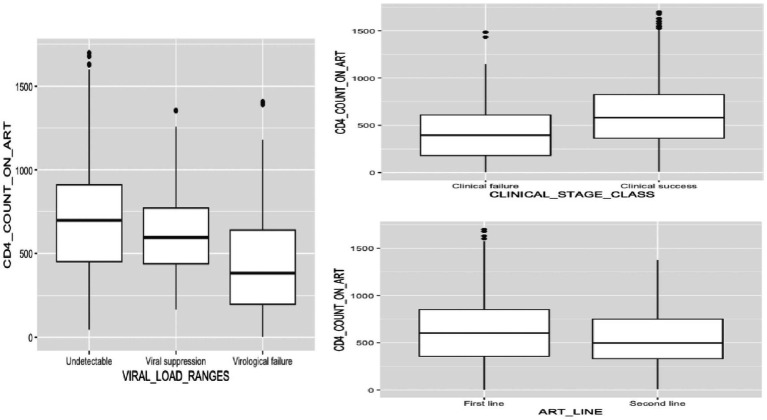
Of the 271 perinatally-infected ALHIV enrolled over three phases, females were predominant (55.7, 55.1, and 56.0%); median age was 14 (IQR: 12-17); majority of the participants were followed-up in urban areas (77.5, 74.5, and 78.6%); and the age distribution favored older adolescents (48.7, 61.2, and 58.5%). Most participants achieved clinical success (93.1, 89.7, 88.9%), predominantly on first-line ART (80.8, 66.2, and 53.0%), with good adherence (64.2, 58.9, and 64.5%). Most participants had secondary education (67.2, 70.1, and 67.5%). Median CD4+ counts fluctuated overtime, with values of 563 (IQR: 249.0-845.0), 502 (IQR: 319.0-783.5), and 628 (IQR: 427.5-817.5), respectively. Of note, being male was linked to a reduction in CD4+ count compared to females, [-200.63 (-379.32 to -21.95), = 0.028]. Similarly, late adolescence was associated with lower CD4+ counts compared to early adolescence, [-181.08 (-301.08 to -61.09), = 0.003]. Moreover, participants experiencing VF showed significantly lower CD4+ counts compared to those with undetectable viral loads, [-353.08 (-465.81 to -240.36), < 0.001]. Additionally, there was a marginally significant interaction between male gender and secondary educational level, [209.78 (-6.94-426.51), = 0.058].
Among perinatally-infected ALHIV, age, gender, educational level, and virological status are key factors influencing their immune health and treatment outcomes. Prioritizing targeted interventions and close monitoring within these subgroups is crucial for optimal management, employing holistic care strategies that consider not only medical interventions but also psychosocial support and education.
在撒哈拉以南非洲地区,感染艾滋病毒的青少年(ALHIV)中与艾滋病相关的死亡率升高受到多种因素影响,尤其是免疫抑制,且治疗选择有限。我们旨在通过评估喀麦隆接受抗逆转录病毒治疗(ART)的围产期感染的ALHIV的免疫反应及相关因素,来加强儿科艾滋病毒的管理。
2018年至2020年在喀麦隆对271名有ART经验的ALHIV进行了一项队列研究。在入组时(T0)、6个月时(T1)和12个月时(T2)分别使用PIMA CD4(雅培/泛泰(私人)有限公司)和雅培应用生物系统平台(实时荧光定量PCR m2000RT)测量社会人口统计学数据、免疫学(CD4)和病毒学(血浆病毒载量,PVL)反应。免疫失败(IF)定义为绝对CD4<250个细胞/mm³,病毒学失败(VF)定义为PVL≥1000拷贝/ml。使用R版本4.4.1的线性混合效应模型估计固定效应和随机效应,显著性设定为<0.05。
在三个阶段入组的271名围产期感染的ALHIV中,女性占主导(分别为55.7%、55.1%和56.0%);中位年龄为14岁(四分位间距:12 - 17岁);大多数参与者在城市地区接受随访(分别为77.5%、74.5%和78.6%);年龄分布有利于年龄较大的青少年(分别为48.7%、61.2%和58.5%)。大多数参与者取得了临床成功(分别为93.1%、89.7%、88.9%),主要接受一线ART治疗(分别为80.8%、66.2%和53.0%),依从性良好(分别为64.2%、58.9%和64.5%)。大多数参与者接受过中等教育(分别为67.2%、70.1%和67.5%)。CD4⁺细胞计数中位数随时间波动,分别为563(四分位间距:249.0 - 845.0)、502(四分位间距:319.0 - 783.5)和628(四分位间距:427.5 - 817.5)。值得注意的是,与女性相比,男性的CD4⁺细胞计数有所下降,[-200.63(-379.32至-21.95),P = 0.028]。同样,与青春期早期相比,青春期晚期的CD4⁺细胞计数较低,[-181.08(-301.08至-61.09),P = 0.003]。此外,与病毒载量不可检测的参与者相比,经历VF的参与者的CD4⁺细胞计数显著更低,[-353.08(-465.81至-240.36),P <0.001]。此外,男性性别与中等教育水平之间存在边缘显著的交互作用,[209.78(-6.94 - 426.51),P = 0.058]。
在围产期感染的ALHIV中,年龄、性别、教育水平和病毒学状态是影响其免疫健康和治疗结果的关键因素。在这些亚组中优先进行有针对性的干预和密切监测对于优化管理至关重要,采用不仅考虑医学干预,还包括心理社会支持和教育的整体护理策略。