Centre de recherche du CHU de Québec - Université Laval (Drolet, Laprise, Chamberland, Sauvageau, Brisson); Département de médecine sociale et préventive (Sauvageau, Brisson), Université Laval; Institut national de santé publique du Québec et Direction régionale de santé publique de la Capitale-Nationale (Sauvageau), Québec, Que.; Public Health Ontario (Wilson, Lim); Dalla Lana School of Public Health (Wilson, Tuite), University of Toronto, Toronto, Ont.; University of British Columbia (Ogilvie), Vancouver, BC; Centre for Immunization Programs (Tuite), Public Health Agency of Canada, Ottawa, Ont.
CMAJ. 2024 Oct 6;196(33):E1136-E1143. doi: 10.1503/cmaj.240787.
Worldwide, countries are examining whether to implement 1-dose human papillomavirus (HPV) vaccination instead of using 2 doses. To inform policy, we sought to project the population-level impact and efficiency of switching from 2-dose to 1-dose gender-neutral routine HPV vaccination in Canada.
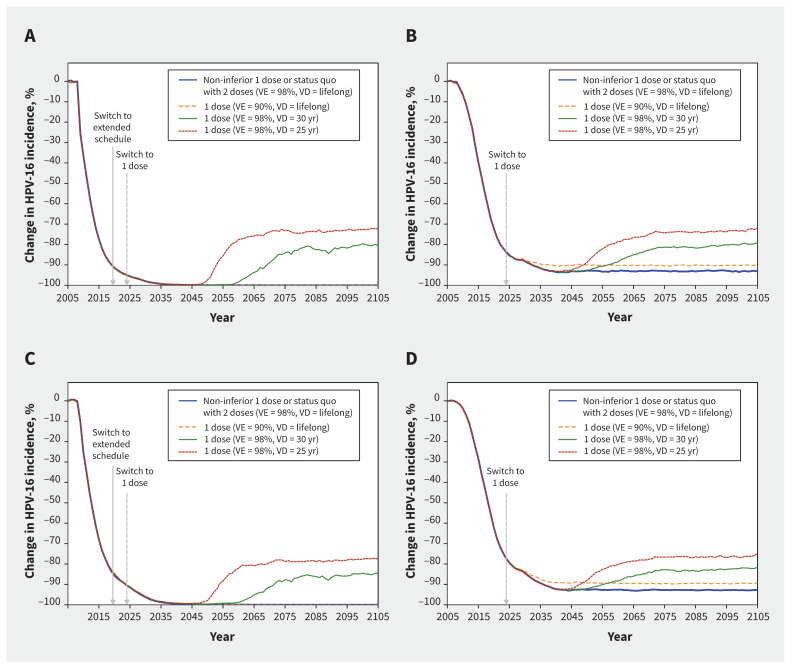
We used HPV-ADVISE, an individual-based transmission-dynamic model of HPV infections and diseases, to mathematically model vaccination programs in 2 provinces, Quebec, a province with high HPV vaccination coverage (around 85%), and Ontario, which has lower coverage (around 65%). We examined non-inferior and pessimistic scenarios of the efficacy (vaccine efficacy of 98% or 90%) and average vaccine duration (lifelong, 30 yr, or 25 yr) of 1 dose compared with 2 doses (98% vaccine efficacy, lifelong vaccine duration). Our main outcomes were the relative reduction in HPV-16 (by sex) and cervical cancers, and the number of doses needed to prevent 1 cervical cancer.
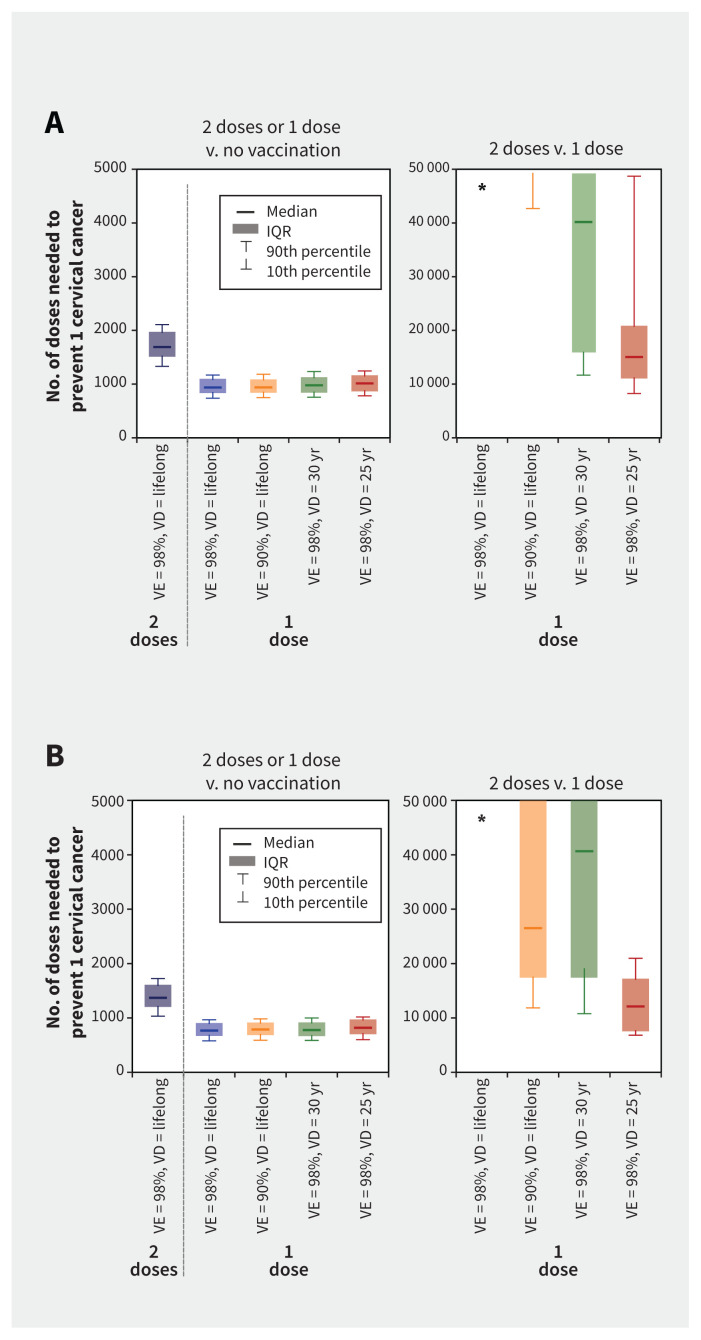
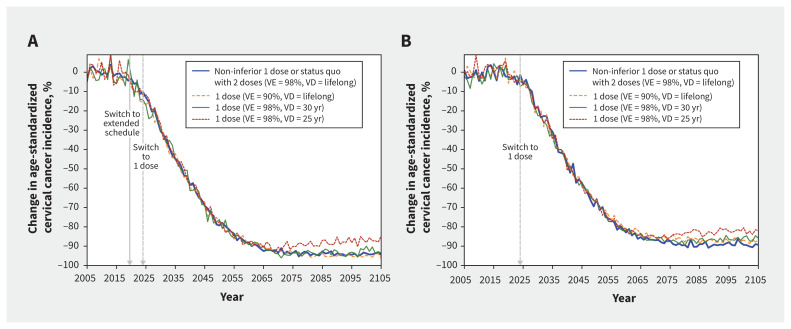
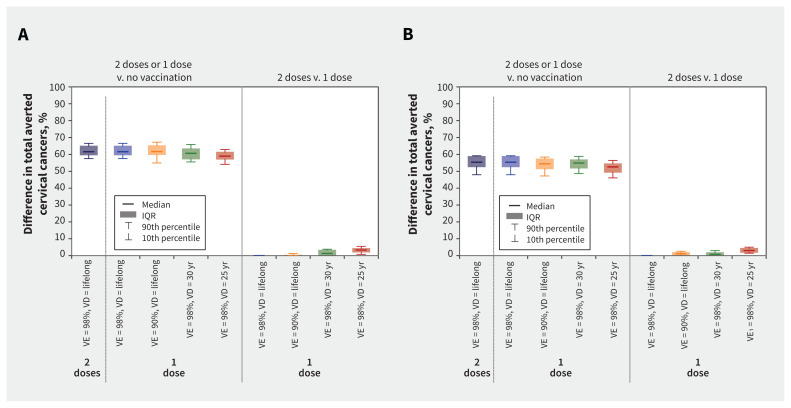
Our model projected that 1-dose HPV vaccination would avert a similar number of cervical cancers as 2 doses in Canada, under various scenarios. Under the most pessimistic scenario (25-yr vaccine duration), 1-dose vaccination would avert fewer cervical cancers than 2 doses, by about 3 percentage points over 100 years. All 1-dose scenarios were projected to lead to elimination of cervical cancer (< 4 cervical cancers/100 000 female-years) and to be a substantially more efficient use of vaccine doses than a 2-dose scenario (1-dose v. no vaccination = 800-1000 doses needed to prevent 1 cervical cancer; incremental doses for 2-dose v. 1-dose vaccination > 10 000 doses needed to prevent 1 additional cervical cancer).
If the average duration of 1-dose protection is longer than 25 years, a 1-dose HPV vaccination program would protect those vaccinated during their peak ages of sexual activity and prevent a similar number of HPV-related cancers as a 2-dose program, while being a more efficient use of vaccine doses.
在全球范围内,各国都在研究是否实施一剂人乳头瘤病毒(HPV)疫苗接种,而不是使用两剂。为了为政策提供信息,我们试图预测在加拿大从两剂转换为一剂性别中立常规 HPV 疫苗接种的人群水平影响和效率。
我们使用 HPV-ADVISE,这是一种 HPV 感染和疾病的基于个体的传播动力学模型,对 2 个省(魁北克省,HPV 疫苗接种覆盖率高(约 85%)和安大略省,疫苗接种覆盖率较低(约 65%)的疫苗接种计划进行数学建模。我们检查了一剂与两剂(疫苗效力 98%,终身疫苗接种持续时间)相比,一剂的效力(疫苗效力为 98%或 90%)和平均疫苗持续时间(终身、30 年或 25 年)的非劣效和悲观情景。我们的主要结果是 HPV-16(按性别)和宫颈癌的相对减少,以及预防 1 例宫颈癌所需的剂量数。
在各种情况下,我们的模型预测,在加拿大,一剂 HPV 疫苗接种将预防与两剂相似数量的宫颈癌。在最悲观的情景(25 年疫苗持续时间)下,一剂疫苗接种在 100 年内将预防宫颈癌的人数比两剂疫苗接种少约 3 个百分点。所有一剂方案都预计将消除宫颈癌(<4 例宫颈癌/100000 名女性年),并且比两剂方案更有效地使用疫苗剂量(一剂与无疫苗接种相比,预防 1 例宫颈癌所需的剂量为 800-1000 剂;2 剂与 1 剂相比,预防 1 例额外宫颈癌所需的增量剂量超过 10000 剂)。
如果一剂保护的平均持续时间超过 25 年,一剂 HPV 疫苗接种计划将保护那些在性活跃高峰期接种疫苗的人,并预防与两剂计划相似数量的 HPV 相关癌症,同时更有效地使用疫苗剂量。