Yoshida Yuriko, Yanagawa Masahiro, Sato Yukihisa, Miyata Tomo, Kawata Atsushi, Hata Akinori, Tomiyama Noriyuki
Department of Diagnostic and Interventional Radiology, Osaka University Graduate School of Medicine, Osaksa, Japan.
Department of Diagnostic Radiology, Suita Municipal Hospital, Osaka, Japan.
Acta Radiol Open. 2024 Oct 4;13(10):20584601241288509. doi: 10.1177/20584601241288509. eCollection 2024 Oct.
There are few CT-based deep learning (DL) studies on thymoma according to the World Health Organization classification.
To develop a CT-based DL model to distinguish between low-risk and high-risk thymoma and to compare the diagnostic performance of radiologists with and without the DL model.
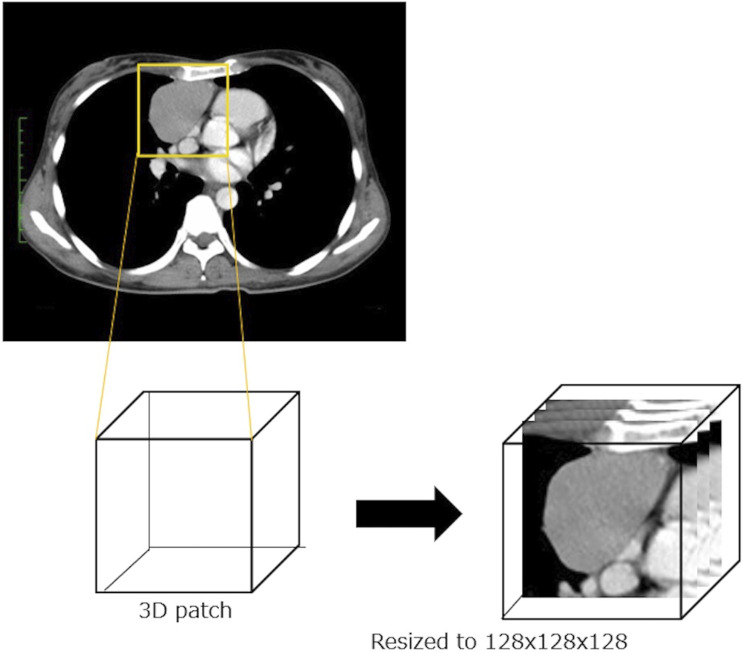
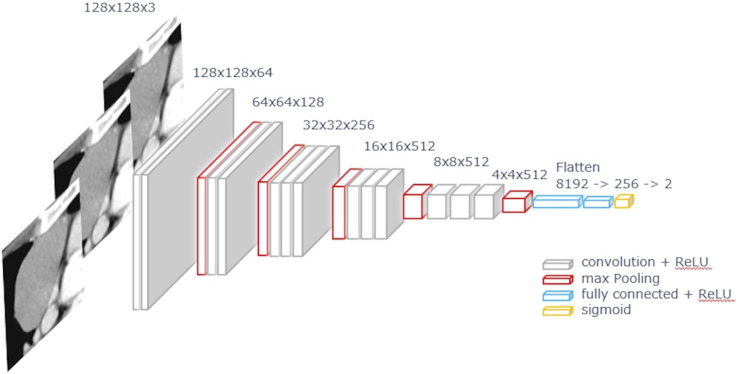
159 patients with 160 thymomas were included. A fine-tuning VGG16 network model with Adam optimizer was used, followed by k-fold cross validation. The dataset consisted of three axial slices, including the maximum tumor size from the CT volume data. The data were augmented 50 times by rotation, zoom, shear, and horizontal/vertical flip. Three independent networks for the CT dataset were considered, and the result was determined by voting. Three radiologists independently diagnosed thymomas with and without the model. The area under the curve (AUC) of the diagnostic performance was compared using receiver operating characteristic analysis.
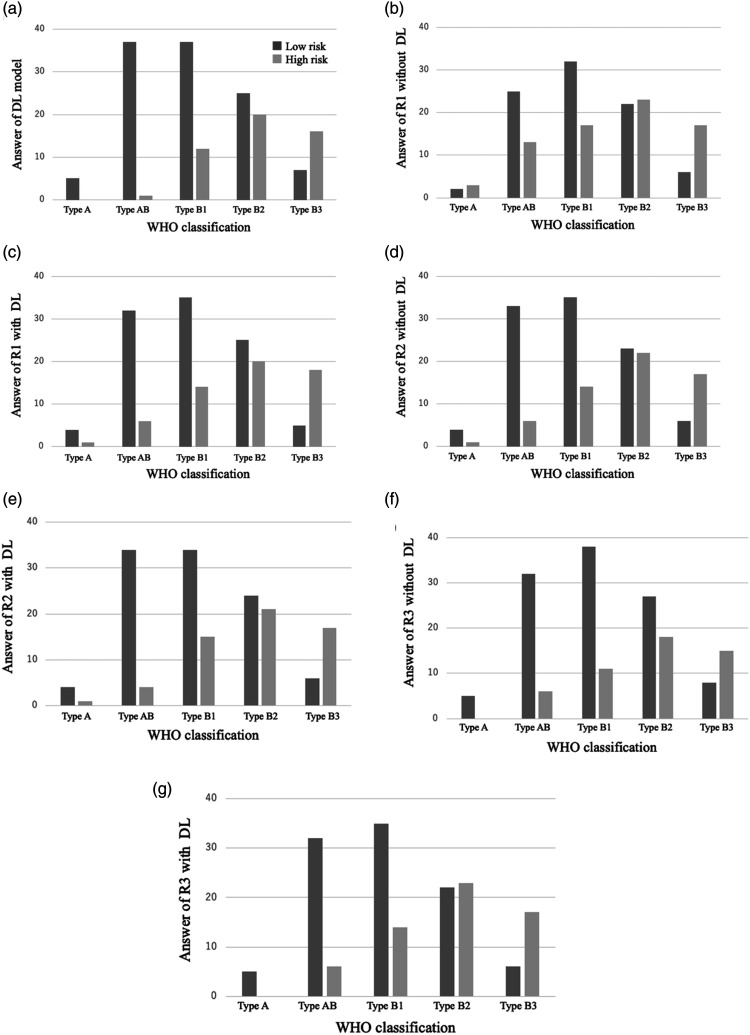
Accuracy of the DL model was 71.3%. Diagnostic performance of the radiologists was as follows: AUC and accuracy without the DL model, 0.61-0.68 and 61.9%-69.3%; and with the DL model, 0.66-0.69 and 68.1%-70.0%, respectively. AUC of the diagnostic performance showed no significant differences between radiologists with and without the DL model. The DL model tended to increase the diagnostic accuracy, but AUC was not significantly improved.
Diagnostic performance of the DL was comparable to that of radiologists. The DL model assistance tended to increase diagnostic accuracy.
根据世界卫生组织的分类,基于CT的深度学习(DL)对胸腺瘤的研究较少。
开发一种基于CT的DL模型,以区分低风险和高风险胸腺瘤,并比较使用和不使用DL模型时放射科医生的诊断性能。
纳入159例患者的160个胸腺瘤。使用带有Adam优化器的微调VGG16网络模型,随后进行k折交叉验证。数据集由三个轴向切片组成,包括来自CT体积数据的最大肿瘤大小。数据通过旋转、缩放、剪切和水平/垂直翻转进行50次增强。考虑了用于CT数据集的三个独立网络,并通过投票确定结果。三位放射科医生分别在有和没有该模型的情况下独立诊断胸腺瘤。使用受试者操作特征分析比较诊断性能的曲线下面积(AUC)。
DL模型的准确率为71.3%。放射科医生的诊断性能如下:不使用DL模型时,AUC和准确率分别为0.61 - 0.68和61.9% - 69.3%;使用DL模型时,分别为0.66 - 0.69和68.1% - 70.0%。有和没有DL模型的放射科医生之间,诊断性能的AUC没有显著差异。DL模型倾向于提高诊断准确性,但AUC没有显著改善。
DL的诊断性能与放射科医生相当。DL模型辅助倾向于提高诊断准确性。