Huele E H, van der Velden J M, Verkooijen H M, Kasperts N, Verlaan J J
Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Department of Radiotherapy, Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Clin Transl Radiat Oncol. 2024 Sep 11;49:100858. doi: 10.1016/j.ctro.2024.100858. eCollection 2024 Nov.
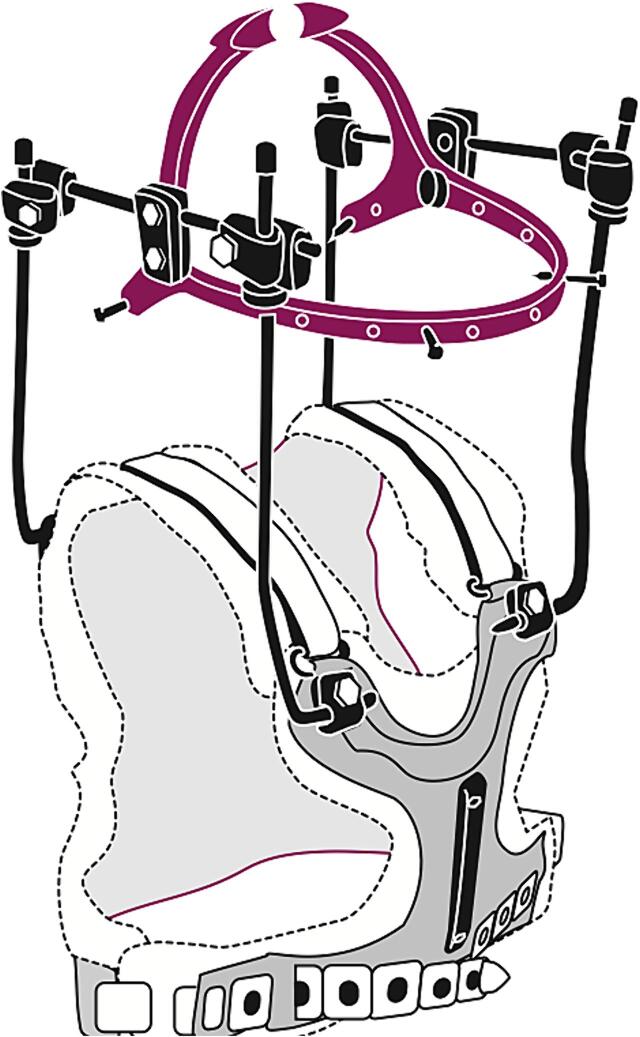
Currently no minimally invasive surgical treatment exists to provide immediate stability for unstable cervical/cervicothoracic metastases. Long-construct spondylodesis carries a high complication risk and has severe impact on residual range of motion. This study explores temporary halo fixation and radiotherapy as an alternative to long-construct cervical spondylodesis.
This retrospective cohort study included twenty patients with multiple unstable cervical metastases treated between 2013-2023. All patients underwent halo fixation for an intended duration of three months to allow for safe reossification of lytic lesions following radiotherapy, with a dose fractionation scheme best suited to the histological origin of the tumor.
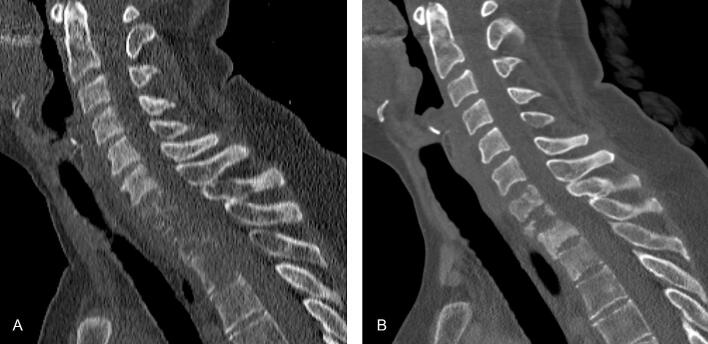
Immobilization with halo fixation lasted a median 83 days (range, 41-132 days). Radiotherapy started on average 7 days after halo fixation (range, -35-118 days). The median pain score at baseline was 8, and was 0 at halo removal and at last follow-up. All patients had no or minor neurological deficits at baseline and did not develop new neurological deficits. At halo removal, 17/18 patients showed radiographic evidence of reossification. The majority of patients experienced minor limitations or had full range of motion of the neck at last follow-up.
Patients with multiple unstable cervical metastases treated with halo fixation and radiotherapy showed complete pain response or substantial pain reduction, reossification of the vertebrae and a, mostly, preserved range of motion. In selected neurologically intact patients, this treatment might be a patient-friendly alternative to fixation. Prospective evaluation of this treatment combination is needed.
目前尚无微创外科治疗方法可为不稳定的颈椎/颈胸段转移瘤提供即时稳定性。长节段脊柱融合术并发症风险高,且对残余活动度有严重影响。本研究探索临时头环固定和放疗作为长节段颈椎脊柱融合术的替代方法。
这项回顾性队列研究纳入了2013年至2023年间接受治疗的20例多发不稳定颈椎转移瘤患者。所有患者均接受了为期三个月的头环固定,以便在放疗后使溶骨性病变安全地重新骨化,放疗的剂量分割方案最适合肿瘤的组织学来源。
头环固定的中位时长为83天(范围41 - 132天)。放疗平均在头环固定后7天开始(范围 - 35 - 118天)。基线时的中位疼痛评分为8分,在去除头环时及末次随访时为0分。所有患者在基线时均无或仅有轻微神经功能缺损,且未出现新的神经功能缺损。在去除头环时,18例患者中有17例显示有重新骨化的影像学证据。大多数患者在末次随访时颈部活动仅有轻微受限或活动范围正常。
接受头环固定和放疗的多发不稳定颈椎转移瘤患者显示出完全的疼痛缓解或疼痛显著减轻、椎体重新骨化,且大部分患者的活动范围得以保留。对于部分神经功能完好的患者,这种治疗可能是一种对患者友好的固定替代方法。需要对这种治疗组合进行前瞻性评估。