Duff Irina T, Likar Rudolf, Perruchoud Christophe, Kampusch Stefan, Köstenberger Markus, Sator Sabine, Stremnitzer Caroline, Wolf Andreas, Neuwersch-Sommeregger Stefan, Abd-Elsayed Alaa
Neurosurgery Department, Johns Hopkins University, Baltimore, MD, USA.
Department for Anesthesia and Critical Care, Klinikum Klagenfurt am Wörthersee, Klagenfurt, Austria.
Pain Ther. 2024 Dec;13(6):1407-1427. doi: 10.1007/s40122-024-00657-8. Epub 2024 Oct 9.
Current guidelines for pain treatment recommend a personalized, multimodal and interdisciplinary approach as well as the use of a combination of drug and non-drug therapies. Risk factors for chronification should already be reduced in patients with acute pain, e.g., after surgery or trauma. Auricular vagus nerve stimulation (aVNS) could be an effective non-drug therapy in the multimodal treatment of chronic and acute pain. The aim of this systematic review and meta-analysis is to evaluate the clinical efficacy and safety of aVNS in treating chronic and acute pain conditions.
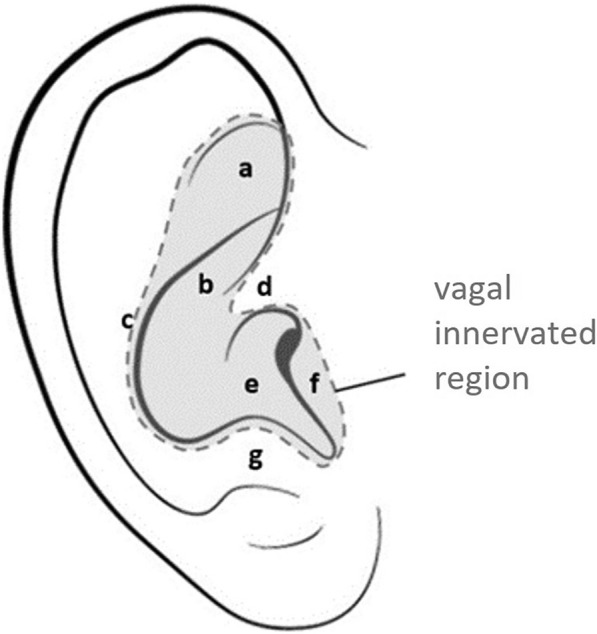
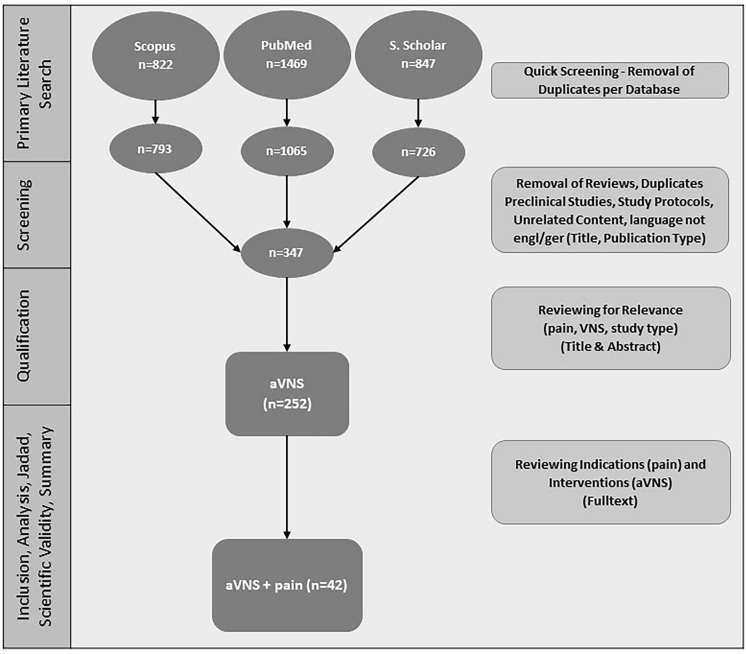
A systematic literature search was performed regarding the application of auricular electrical stimulation in chronic and acute pain. Studies were classified according to their level of evidence (Jadad scale), scientific validity and risk of bias (RoB 2 tool) and analyzed regarding indication, method, stimulation parameters, duration of treatment and efficacy and safety. A meta-analysis on (randomized) controlled trials (using different comparators) was performed for chronic and acute pain conditions, respectively, including subgroup analysis for percutaneous (pVNS-needle electrodes) and transcutaneous (tVNS-surface electrodes) aVNS. The visual analog pain scale (VAS) was defined as primary efficacy endpoint.
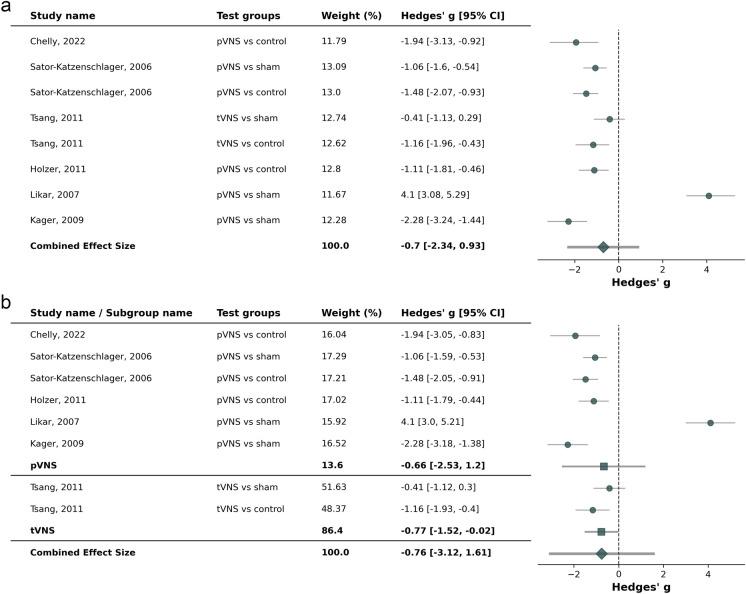
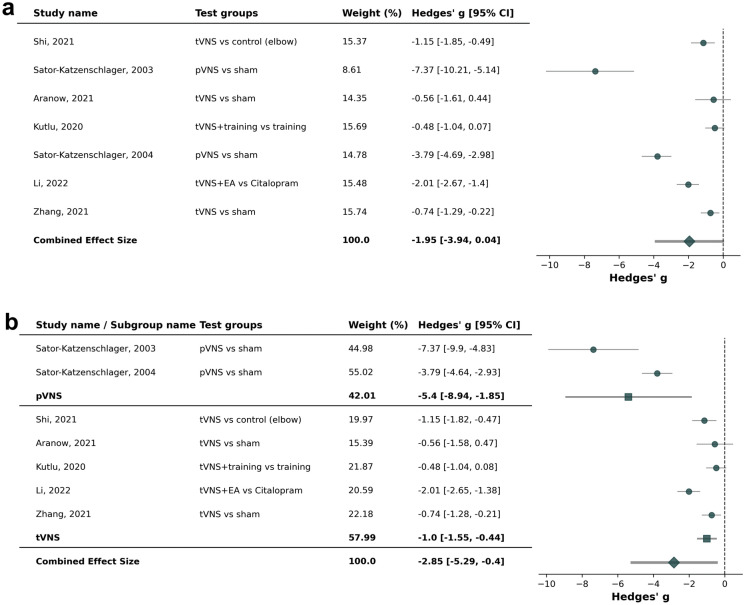
A total of n = 1496 patients were treated with aVNS in 23 identified and analyzed studies in chronic pain, 12 studies in acute postoperative pain and 7 studies in experimental acute pain. Of these, seven studies for chronic pain and six studies for acute postoperative pain were included in the meta-analysis. In chronic pain conditions, including back pain, migraine and abdominal pain, a statistically significant reduction in VAS pain intensity for active compared to sham aVNS or control treatment with an effect size Hedges' g/mean difference of - 1.95 (95% confidence interval [CI]: - 3.94 to 0.04, p = 0.008) could be shown and a more favorable effect in pVNS compared to tVNS (- 5.40 [- 8.94; - 1.85] vs. - 1.00 [- 1.55; - 0.44]; p = 0.015). In acute pain conditions, single studies showed significant improvements with aVNS, e.g., in kidney donor surgery or tonsillectomy but, overall, a non-statistically significant reduction in VAS pain intensity for active compared to sham aVNS or control with - 0.70 [- 2.34; 0.93] (p = 0.15) could be observed in the meta-analysis. In acute pain results vary greatly between studies depending especially on co-medication and timepoints of assessment after surgery. A significant reduction in analgesics or opiate intake was documented in most studies evaluating this effect in chronic and acute pain. In 3 of the 12 randomized controlled trials in patients with chronic pain, a sustainable pain reduction over a period of up to 12 months was shown. Overall, aVNS was very well tolerated.
This systematic review and meta-analysis indicate that aVNS can be an effective and safe non-drug treatment in patients with specific chronic and acute postoperative pain conditions. Further research is needed to identify the influence of simulation parameters and find optimal and standardized treatment protocols while considering quality-of-life outcome parameters and prolonged follow-up periods. A more standardized approach and harmonization in study designs would improve comparability and robustness of outcomes.
当前的疼痛治疗指南推荐采用个性化、多模式和跨学科的方法,以及药物和非药物疗法相结合的方式。对于急性疼痛患者,如术后或创伤后患者,应减少慢性化的风险因素。耳迷走神经刺激(aVNS)可能是慢性和急性疼痛多模式治疗中一种有效的非药物疗法。本系统评价和荟萃分析的目的是评估aVNS治疗慢性和急性疼痛的临床疗效和安全性。
针对耳电刺激在慢性和急性疼痛中的应用进行了系统的文献检索。根据证据水平(Jadad量表)、科学有效性和偏倚风险(RoB 2工具)对研究进行分类,并对适应症、方法、刺激参数、治疗持续时间以及疗效和安全性进行分析。分别对慢性和急性疼痛情况进行了(随机)对照试验的荟萃分析(使用不同的对照),包括经皮(pVNS-针电极)和经皮(tVNS-表面电极)aVNS的亚组分析。视觉模拟疼痛量表(VAS)被定义为主要疗效终点。
在23项已确定并分析的慢性疼痛研究、12项急性术后疼痛研究和7项实验性急性疼痛研究中,共有n = 1496例患者接受了aVNS治疗。其中,荟萃分析纳入了7项慢性疼痛研究和6项急性术后疼痛研究。在慢性疼痛情况下,包括背痛、偏头痛和腹痛,与假aVNS或对照治疗相比,主动治疗的VAS疼痛强度在统计学上有显著降低,效应大小Hedges' g/平均差为 -1.95(95%置信区间[CI]:-3.94至0.04,p = 0.008),并且与tVNS相比,pVNS的效果更优(-5.40 [-8.94;-1.85] 对 -1.00 [-1.55;-0.44];p = 0.015)。在急性疼痛情况下,个别研究显示aVNS有显著改善,例如在肾移植手术或扁桃体切除术中,但总体而言,荟萃分析显示与假aVNS或对照相比,主动治疗的VAS疼痛强度无统计学意义的降低,为 -0.70 [-2.34;0.93](p = 0.15)。在急性疼痛中,研究结果差异很大,尤其取决于联合用药和术后评估时间点。在大多数评估慢性和急性疼痛中这种效果的研究中,均记录到镇痛药或阿片类药物摄入量显著减少。在12项慢性疼痛患者的随机对照试验中,有3项显示长达12个月的持续疼痛缓解。总体而言,aVNS耐受性良好。
本系统评价和荟萃分析表明,aVNS在特定慢性和急性术后疼痛患者中可以是一种有效且安全的非药物治疗方法。需要进一步研究以确定模拟参数的影响,并在考虑生活质量结果参数和延长随访期的同时找到最佳和标准化的治疗方案。研究设计中更标准化的方法和协调将提高结果的可比性和稳健性。