Department of Radiation Oncology, Cancer Institute, IKHC, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Radiation Oncology Research Center, Cancer Research Institute, IKHC, Tehran University of Medical Sciences, Tehran, Iran.
Cancer Med. 2024 Oct;13(19):e70291. doi: 10.1002/cam4.70291.
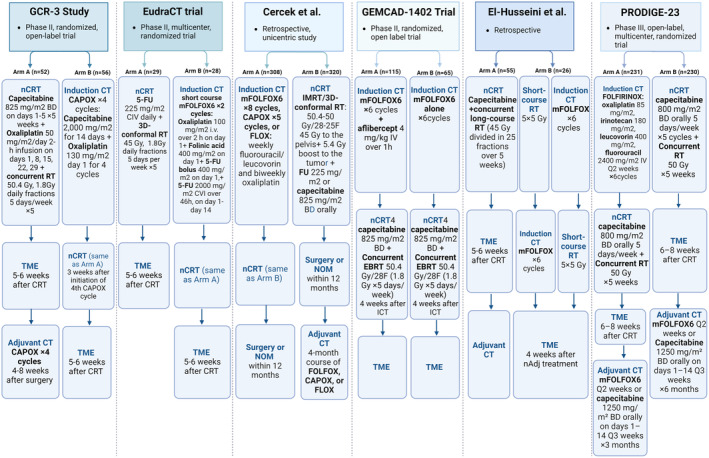
Historically, multimodal therapeutic strategies involving preoperative chemoradiotherapy (CRT), surgery, and adjuvant chemotherapy (CT) have been employed to treat locally advanced rectal cancer (LARC). Total Neoadjuvant Therapy (TNT) is showing promise in improving outcomes. Despite its benefits, the optimal sequencing within TNT-whether induction chemotherapy should precede or follow chemoradiotherapy-remains a critical question. This study endeavors to explore the effects of different TNT sequencing strategies on patient outcomes, including tumor downstaging, pathological response, organ preservation, and the balance between efficacy and tolerability.
Our methodology entailed a comprehensive literature review conducted on Medline, focusing on recent research, including retrospective studies, systematic reviews, and clinical trials. The review emphasized the comparison of induction chemotherapy versus consolidation chemotherapy within TNT regimens, assessing outcomes such as pathological response, organ preservation rates, and adverse effects. To ensure the selection of appropriate and high-quality studies, specific inclusion and exclusion criteria were applied.
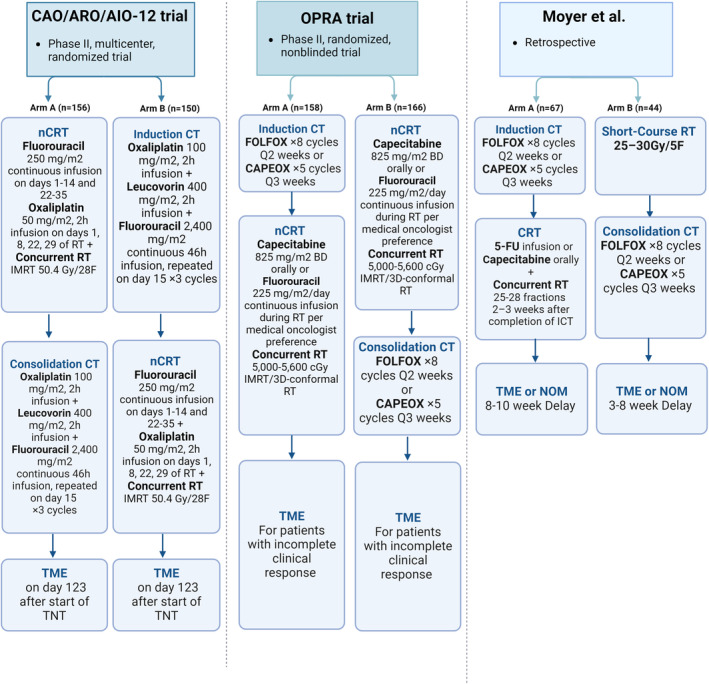
The analysis revealed that induction chemotherapy might lead to decreased adherence to subsequent chemoradiotherapy while offering an early intervention against micrometastasis and potentially improving overall chemotherapy compliance. Conversely, consolidation chemotherapy has been associated with higher pathological complete response (pCR) rates and improved tolerability, indicating its potential for patients requiring local symptom relief or those eligible for a nonoperative management approach. Comparative studies like CAO/ARO/AIO-12 and the OPRA trials have significantly contributed to our understanding, suggesting that while both strategies have distinct advantages, the choice between induction and consolidation chemotherapy should be tailored based on individual patient profiles and tumor characteristics.
This narrative review underscores the importance of a nuanced approach to TNT sequencing in locally advanced rectal cancer, highlighting the need for further research to refine treatment strategies.
历史上,采用术前放化疗(CRT)、手术和辅助化疗(CT)的多模态治疗策略来治疗局部晚期直肠癌(LARC)。全新辅助治疗(TNT)在改善疗效方面显示出前景。
尽管有其益处,但 TNT 内的最佳排序 - 诱导化疗是否应先于放化疗或后于放化疗 - 仍然是一个关键问题。本研究旨在探讨不同 TNT 排序策略对患者结局的影响,包括肿瘤降期、病理缓解、器官保存以及疗效和耐受性之间的平衡。
我们的方法是在 Medline 上进行全面的文献综述,重点关注最近的研究,包括回顾性研究、系统评价和临床试验。
该综述强调了 TNT 方案中诱导化疗与巩固化疗的比较,评估了病理缓解、器官保存率和不良反应等结局。
为了确保选择适当和高质量的研究,应用了特定的纳入和排除标准。
分析表明,诱导化疗可能会导致随后接受放化疗的患者减少,而早期干预微转移并可能提高整体化疗依从性。
相反,巩固化疗与较高的病理完全缓解(pCR)率和改善的耐受性相关,表明其对需要局部症状缓解或适合非手术管理方法的患者具有潜力。
CAO/ARO/AIO-12 和 OPRA 试验等比较研究极大地促进了我们的理解,表明虽然这两种策略都有明显的优势,但诱导和巩固化疗之间的选择应根据患者个体特征和肿瘤特征量身定制。