Department of General Practice and Health Services Research, Section for Health Equity Studies & Migration, Heidelberg University Hospital, Im Neuenheimer Feld 130.3, Heidelberg, 69120, Germany.
Department of Population Medicine and Health Services Research, School of Public Health, University of Bielefeld, Universitätsstraße 25, Bielefeld, 33615, Germany.
Int J Equity Health. 2024 Oct 10;23(1):208. doi: 10.1186/s12939-024-02251-y.
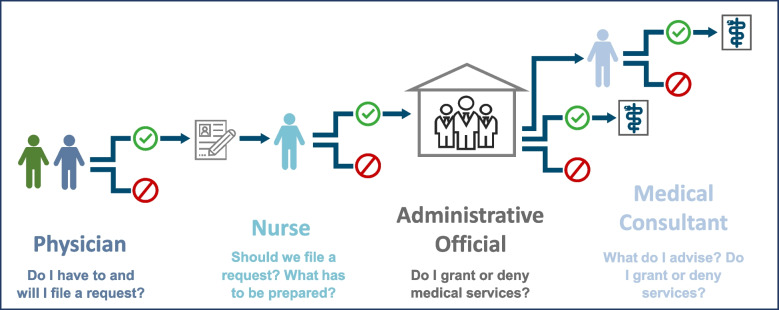
Access to health services for asylum seekers is legally restricted in Germany. The law is subject to interpretation, therefore the chance of receiving care is not equally distributed among asylum seekers. What services are provided to whom is ultimately decided by health professionals and government employees. The respective prioritization processes and criteria are not transparent. We sought to understand how legal restrictions are translated into daily practices and how this affects the health system. We aimed to outline the complex process of cost coverage for health services for asylum seekers and provide insights into common decision-making criteria.
We conducted an ethnographic exploration of routines in two outpatient clinics in two federal states over the course of three months, doing participant and non-participant observation. Additionally, we interviewed 21 professionals of health care and government organizations, and documented 110 applications for cost coverage of medical services and their outcome. In addition to qualitative data analysis and documentation, we apply a system-theoretical perspective to our findings.
To perform legal restrictions a cross-sectoral prioritization process of medical services has been implemented, involving health care and government institutions. This changes professional practices, responsibilities and (power) relations. Involved actors find themselves at the intersection of several, oftentimes conflicting priorities, since "doing it right" might be seen differently from a legal, medical, economic, or political perspective. The system-theoretical analysis reveals that while actors have to bring different rationales into workable arrangements this part of the medical system transforms, giving rise to a sub-system that incorporates migration political rationales.
Health care restrictions for asylum seekers are implemented through an organizational linking of care provision and government administration, resulting in a bureaucratization of practice. Power structures at this intersection of health and migration policy, that are uncommon in other parts of the health system are thereby normalized. Outpatient clinics provide low-threshold access to health services, but paradoxically they may unintentionally stabilize health inequities, if prioritization criteria and power dynamics are not made transparent. Health professionals should openly reflect on conflicting rationales. Training, research and professional associations need to empower them to stay true to professional ethical principles and international conventions.
在德国,寻求庇护者获得医疗服务的机会受到法律限制。该法律可被解释,因此寻求庇护者获得医疗服务的机会并不均等。谁能获得哪些服务最终由卫生专业人员和政府雇员决定。各自的优先排序过程和标准不透明。我们试图了解法律限制如何转化为日常实践,以及这如何影响卫生系统。我们旨在概述为寻求庇护者的医疗服务提供费用覆盖的复杂过程,并提供常见决策标准的见解。
我们在两个联邦州的两家门诊诊所进行了为期三个月的人种学探索,进行了参与者和非参与者观察。此外,我们采访了 21 名医疗保健和政府组织的专业人员,并记录了 110 份医疗服务费用覆盖申请及其结果。除了定性数据分析和记录外,我们还将系统理论视角应用于我们的发现。
为了执行法律限制,已经实施了医疗服务的跨部门优先排序过程,涉及医疗保健和政府机构。这改变了专业实践、责任和(权力)关系。相关行为者发现自己处于几个相互冲突的优先事项的交叉点,因为“正确行事”可能从法律、医疗、经济或政治角度有不同的看法。系统理论分析表明,虽然行为者必须将不同的推理纳入可行的安排中,但这部分医疗系统会发生转变,形成一个包含移民政治推理的子系统。
对寻求庇护者的医疗保健限制是通过提供医疗服务和政府管理的组织联系来实施的,从而导致实践的官僚化。在卫生和移民政策的交叉点上的权力结构在卫生系统的其他部分并不常见,因此变得正常化。门诊诊所提供低门槛的医疗服务,但如果不透明优先排序标准和权力动态,它们可能会无意中稳定健康不平等。卫生专业人员应该公开反思相互冲突的推理。培训、研究和专业协会需要赋予他们权力,使他们能够坚持专业伦理原则和国际公约。