Division of Biliary Surgery, Department of General Surgery, West China Hospital, Sichuan University, Chengdu, 610041, Sichuan, China.
Department of Oncology and the Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University School of Medicine, 1650 Orleans St, Baltimore, MD, 21287, USA.
J Hematol Oncol. 2024 Oct 10;17(1):92. doi: 10.1186/s13045-024-01613-x.
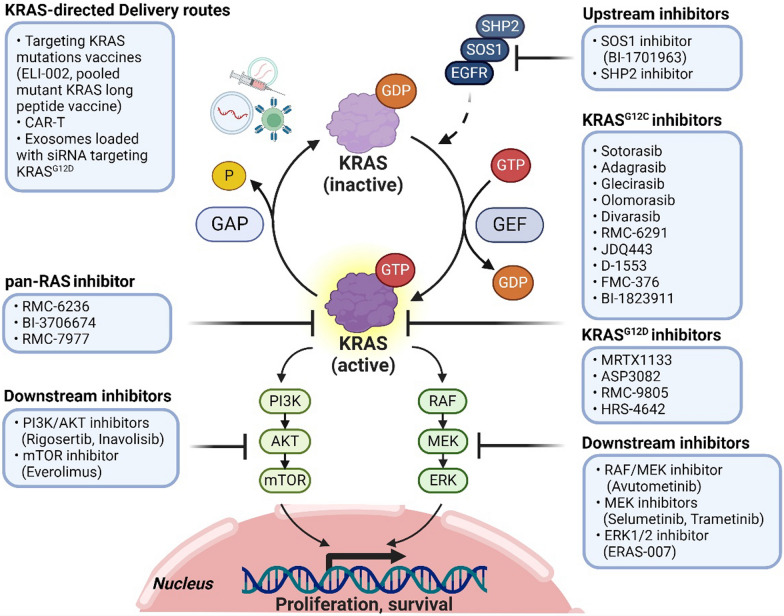
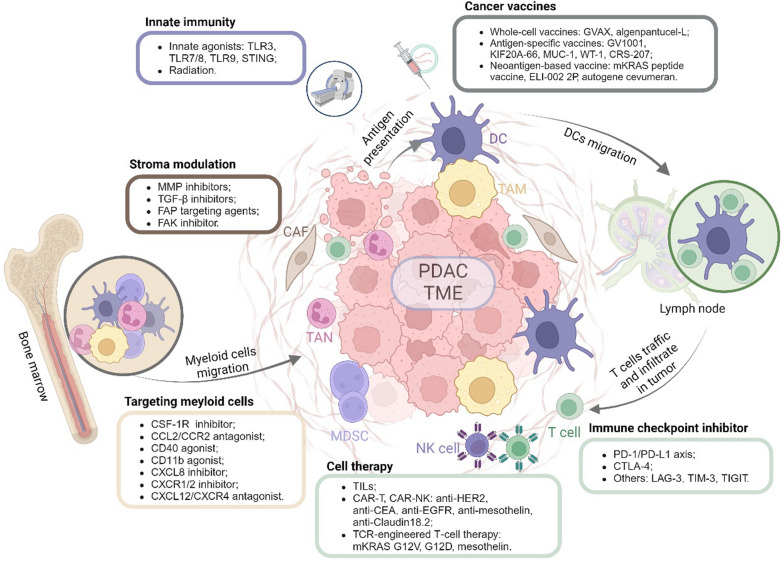
Pancreatic cancer remains one of the most aggressive solid tumors. As a systemic disease, despite the improvement of multi-modality treatment strategies, the prognosis of pancreatic cancer was not improved dramatically. For resectable or borderline resectable patients, the surgical strategy centered on improving R0 resection rate is consensus; however, the role of neoadjuvant therapy in resectable patients and the optimal neoadjuvant therapy of chemotherapy with or without radiotherapy in borderline resectable patients were debated. Postoperative adjuvant chemotherapy of gemcitabine/capecitabine or mFOLFIRINOX is recommended regardless of the margin status. Chemotherapy as the first-line treatment strategy for advanced or metastatic patients included FOLFIRINOX, gemcitabine/nab-paclitaxel, or NALIRIFOX regimens whereas 5-FU plus liposomal irinotecan was the only standard of care second-line therapy. Immunotherapy is an innovative therapy although anti-PD-1 antibody is currently the only agent approved by for MSI-H, dMMR, or TMB-high solid tumors, which represent a very small subset of pancreatic cancers. Combination strategies to increase the immunogenicity and to overcome the immunosuppressive tumor microenvironment may sensitize pancreatic cancer to immunotherapy. Targeted therapies represented by PARP and KRAS inhibitors are also under investigation, showing benefits in improving progression-free survival and objective response rate. This review discusses the current treatment modalities and highlights innovative therapies for pancreatic cancer.
胰腺癌仍然是最具侵袭性的实体肿瘤之一。作为一种全身性疾病,尽管多模式治疗策略有所改善,但胰腺癌的预后并未显著改善。对于可切除或交界可切除的患者,以提高 R0 切除率为中心的手术策略是共识;然而,新辅助治疗在可切除患者中的作用以及化疗联合或不联合放疗的交界可切除患者的最佳新辅助治疗方案仍存在争议。无论切缘状态如何,术后吉西他滨/卡培他滨或 mFOLFIRINOX 辅助化疗均被推荐。对于晚期或转移性患者,化疗作为一线治疗策略包括 FOLFIRINOX、吉西他滨/白蛋白紫杉醇或 NALIRIFOX 方案,而 5-FU 加脂质体伊立替康是唯一的二线治疗标准。免疫疗法是一种创新疗法,尽管抗 PD-1 抗体是目前唯一被批准用于 MSI-H、dMMR 或 TMB-高的实体肿瘤的药物,而这些肿瘤仅占胰腺癌的一小部分。增加免疫原性和克服免疫抑制肿瘤微环境的联合策略可能使胰腺癌对免疫疗法敏感。以 PARP 和 KRAS 抑制剂为代表的靶向治疗也在研究中,显示出改善无进展生存期和客观缓解率的益处。本文讨论了目前的治疗方法,并强调了胰腺癌的创新疗法。