Sarah Cannon Research Institute UK, London, UK.
Early Drug Development and Breast Medicine Services, Division of Solid Tumor Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
J Natl Cancer Inst. 2024 Sep 1;116(9):1439-1449. doi: 10.1093/jnci/djae098.
Camonsertib is a selective oral inhibitor of ataxia telangiectasia and Rad3-related (ATR) kinase with demonstrated efficacy in tumors with DNA damage response gene deficiencies. On-target anemia is the main drug-related toxicity typically manifesting after the period of dose-limiting toxicity evaluation. Thus, dose and schedule optimization requires extended follow-up to assess prolonged treatment effects.
Long-term safety, tolerability, and antitumor efficacy of 3 camonsertib monotherapy dosing regimens were assessed in the TRESR study dose-optimization phase: 160 mg once daily (QD) 3 days on, 4 days off (160 3/4; the preliminary recommended Phase II dose [RP2D]) and two step-down groups of 120 mg QD 3/4 (120 3/4) and 160 mg QD 3/4, 2 weeks on, 1 week off (160 3/4, 2/1w). Safety endpoints included incidence of treatment-related adverse events (TRAEs), dose modifications, and transfusions. Efficacy endpoints included overall response rate, clinical benefit rate, progression-free survival, and circulating tumor DNA (ctDNA)-based molecular response rate.
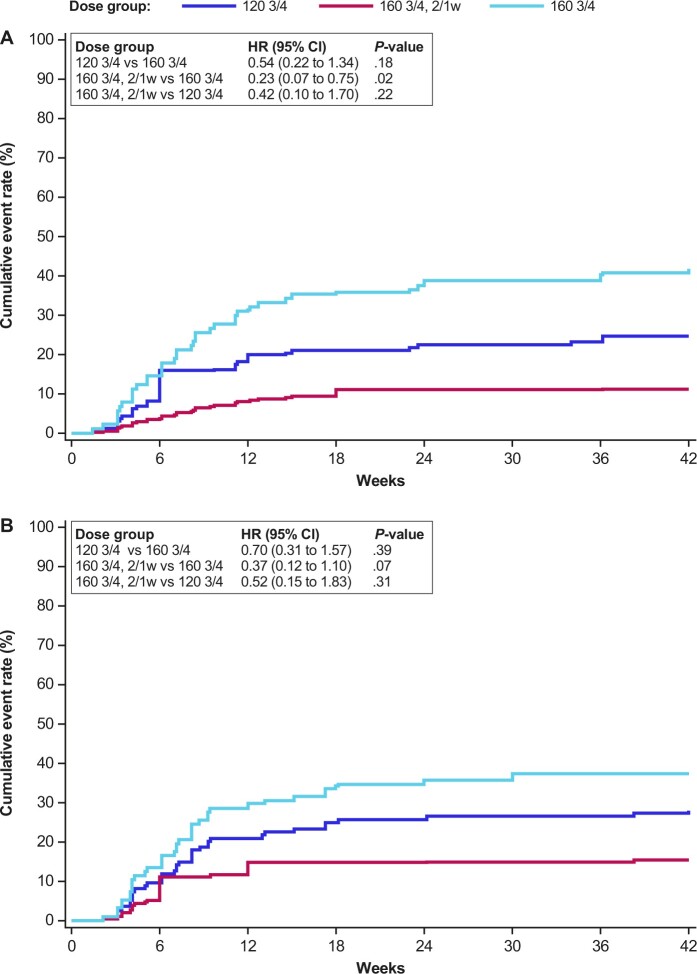
The analysis included 119 patients: 160 3/4 (n = 67), 120 3/4 (n = 25), and 160 3/4, 2/1w (n = 27) treated up to 117.1 weeks as of the data cutoff. The risk of developing grade 3 anemia was significantly lower in the 160 3/4, 2/1w group compared with the preliminary RP2D group (hazard ratio = 0.23, 2-sided P = .02), translating to reduced transfusion and dose reduction requirements. The intermittent weekly schedule did not compromise antitumor activity.
The 160 3/4, 2/1w dose was established as an optimized regimen for future camonsertib monotherapy studies offering a substantial reduction in the incidence of anemia without any compromise to efficacy.
NCT04497116.
卡莫司替尼是一种选择性口服的共济失调毛细血管扩张症和 Rad3 相关(ATR)激酶抑制剂,在 DNA 损伤反应基因缺陷的肿瘤中显示出疗效。靶标相关性贫血是主要的药物相关毒性,通常在剂量限制毒性评估期过后表现出来。因此,需要进行扩展随访以评估延长治疗效果,从而优化剂量和方案。
在 TRESR 研究剂量优化阶段,评估了 3 种卡莫司替尼单药治疗方案的长期安全性、耐受性和抗肿瘤疗效:160mg 每日一次(QD),连续用药 3 天,停药 4 天(160 3/4;初步推荐的 II 期剂量[RP2D])和两个剂量下调组,即 120mg QD 3/4(120 3/4)和 160mg QD 3/4,连续用药 2 周,停药 1 周(160 3/4,2/1w)。安全性终点包括治疗相关不良事件(TRAEs)的发生率、剂量调整和输血。疗效终点包括总缓解率、临床获益率、无进展生存期和循环肿瘤 DNA(ctDNA)的分子缓解率。
分析纳入了 119 例患者:160 3/4(n=67)、120 3/4(n=25)和 160 3/4,2/1w(n=27),截至数据截止日期,分别接受治疗 117.1 周。与初步 RP2D 组相比,160 3/4,2/1w 组发生 3 级贫血的风险显著降低(风险比=0.23,双侧 P=0.02),这意味着输血和剂量减少的需求降低。每周间歇方案并未影响抗肿瘤活性。
160 3/4,2/1w 剂量方案被确立为未来卡莫司替尼单药治疗研究的优化方案,可显著降低贫血的发生率,同时不影响疗效。
NCT04497116。