Hussein Mostafa M, Amer Akram M, Maarouf Mohammed M
Department of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
J Anaesthesiol Clin Pharmacol. 2024 Jul-Sep;40(3):403-409. doi: 10.4103/joacp.joacp_113_23. Epub 2023 Aug 16.
Pediatric upper gastrointestinal (GI) endoscopy is commonly performed under deep sedation, which is frequently associated with respiratory complications. The study compared the respiratory benefits of applying bilateral modified nasopharyngeal airways (NPAs) to conventional low-flow nasal cannula (LFNC).
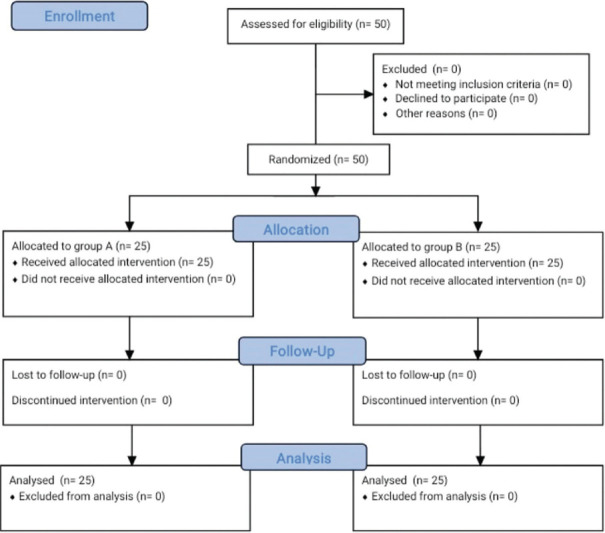
Fifty patients scheduled for an upper GI endoscopy under deep sedation, with an American Society of Anesthesiologists physical status I/II, were enrolled in the study. The patients were randomly divided into bilateral NPA group and the LFNC group. Fentanyl and propofol were administered to both groups to maintain deep sedation. After the application of NPA or LFNC, the hypoxic incidents (oxygen saturation [SpO] <90%) and airway interventions during the procedure were noted and recorded. Other outcomes such as nasopharyngeal injuries, gastroenterologist satisfaction, the incidence of hypotension or bradycardia, and postoperative nausea and vomiting were also compared.
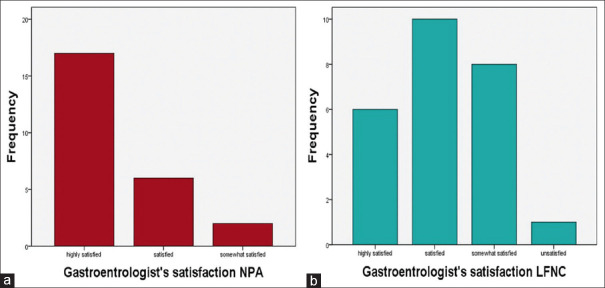
No significant differences were noted in the demographic data. The incidence of hypoxemia was 16% ( = 4) in the NPA group versus 36% ( = 9) in the LFNC group ( = 0.634). Airway intervention was lower in the NPA group compared to the LFNC group, but the difference was not significant ( = 0.539). No significant differences were noted in the incidence of nasopharyngeal injuries, postoperative nausea and vomiting, bradycardia, and hypotension. The NPA group showed higher gastroenterologist's satisfaction ( = 0.003).
Double-modified NPA in pediatric endoscopy was noninferior to the standard LFNC for the incidence of hypoxemia and airway intervention rate, with greater gastroenterologist satisfaction.
小儿上消化道(GI)内镜检查通常在深度镇静下进行,这常与呼吸并发症相关。本研究比较了应用双侧改良鼻咽通气道(NPAs)与传统低流量鼻导管(LFNC)的呼吸益处。
五十例计划在深度镇静下进行上消化道内镜检查、美国麻醉医师协会身体状况分级为I/II级的患者纳入本研究。患者被随机分为双侧NPAs组和LFNC组。两组均给予芬太尼和丙泊酚以维持深度镇静。在应用NPAs或LFNC后,记录操作过程中的低氧事件(血氧饱和度[SpO] <90%)和气道干预情况。还比较了其他结果,如鼻咽部损伤、胃肠病学家满意度、低血压或心动过缓的发生率以及术后恶心和呕吐情况。
两组患者的人口统计学数据无显著差异。NPAs组低氧血症发生率为16%(n = 4),LFNC组为36%(n = 9)(P = 0.634)。NPAs组的气道干预低于LFNC组,但差异无统计学意义(P = 0.539)。鼻咽部损伤、术后恶心和呕吐、心动过缓和低血压的发生率无显著差异。NPAs组的胃肠病学家满意度更高(P = 0.003)。
在小儿内镜检查中,双侧改良NPAs在低氧血症发生率和气道干预率方面不劣于标准LFNC,且胃肠病学家满意度更高。