Department of Tumor Pathology, Hamamatsu University School of Medicine, 1-20-1 Handayama, Chuo-ku, Hamamatsu, Shizuoka, 431-3192, Japan.
Department of Biomedical Laboratory Sciences, School of Health Sciences, College of Medicine and Health Sciences, University of Rwanda, P.O. Box 3286, Kigali, Rwanda.
BMC Cancer. 2024 Oct 11;24(1):1266. doi: 10.1186/s12885-024-13009-8.
Mutations in the TP53 tumor suppressor gene are well-established drivers of colorectal cancer (CRC) development. However, data on the prevalence of TP53 variants and their association with consensus molecular subtype (CMS) classification in patients with CRC from Rwanda are currently lacking. This study addressed this knowledge gap by investigating TP53 mutation status concerning CMS classification in a CRC cohort from Rwanda.
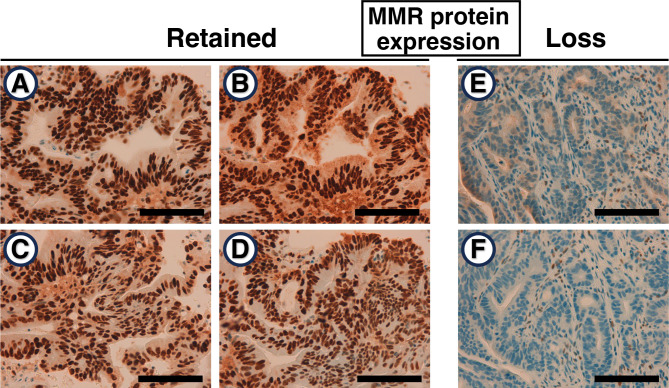
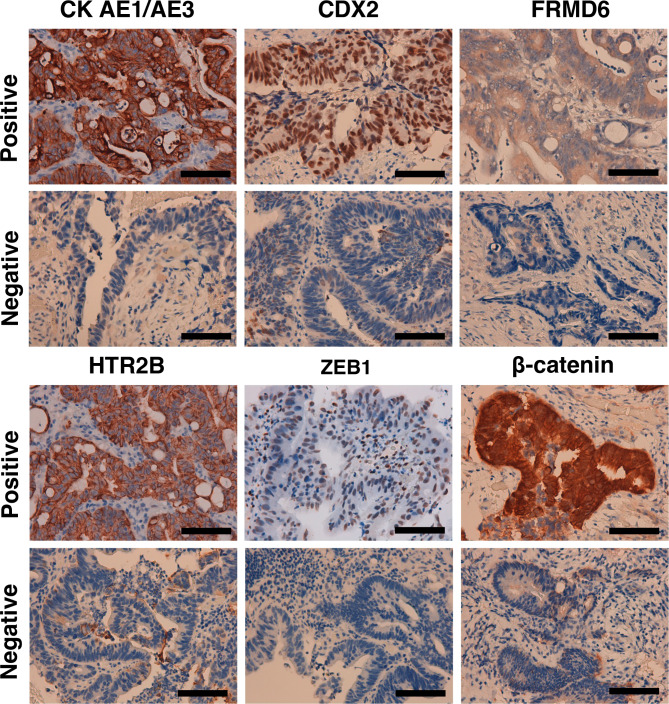
Formalin-fixed paraffin-embedded (FFPE) tissue blocks were obtained from 51 patients with CRC at the University Teaching Hospital of Kigali, Rwanda. Exons 4 to 11 and their flanking intron-exon boundaries in the TP53 gene were sequenced using Sanger sequencing to identify potential variants. The recently established immunohistochemistry-based classifier was employed to determine the CMS of each tumor.
Sequencing analysis of cancerous tissue DNA revealed TP53 pathogenic variants in 23 of 51 (45.1%) patients from Rwanda. These variants were predominantly missense types (18/23, 78.3%). The most frequent were c.455dup (p.P153Afs*28), c.524G > A (p.R175H), and c.733G > A (p.G245S), each identified in three tumors. Trinucleotide sequence context analysis of the 23 mutations (20 of which were single-base substitutions) revealed a predominance of the [C > N] pattern among single-base substitutions (SBSs) (18/20; 90.0%), with C[C > T]G being the most frequent mutation (5/18, 27.8%). Furthermore, pyrimidine bases (C and T) were preferentially found at the 5' flanking position of the mutated cytosine (13/18; 72.2%). Analysis of CMS subtypes revealed the following distribution: CMS1 (microsatellite instability-immune) (6/51, 11.8%), CMS2 (canonical) (28/51, 54.9%), CMS3 (metabolic) (9/51, 17.6%), and CMS4 (mesenchymal) (8/51, 15.7%). Interestingly, the majority of TP53 variants were in the CMS2 subgroup (14/23; 60.1%).
Our findings indicate a high frequency of TP53 variants in CRC patients from Rwanda. Importantly, these variants are enriched in the CMS2 subtype. This study, representing the second investigation into molecular alterations in patients with CRC from Rwanda and the first to explore TP53 mutations and CMS classification, provides valuable insights into the molecular landscape of CRC in this understudied population.
TP53 肿瘤抑制基因的突变是结直肠癌(CRC)发展的公认驱动因素。然而,目前卢旺达 CRC 患者中 TP53 变体的流行率及其与共识分子亚型(CMS)分类的关联的数据尚不清楚。本研究通过调查卢旺达 CRC 队列中 TP53 突变状态与 CMS 分类,填补了这一知识空白。
从卢旺达基加利大学教学医院获得 51 名 CRC 患者的福尔马林固定石蜡包埋(FFPE)组织块。使用 Sanger 测序对 TP53 基因的外显子 4 至 11 及其侧翼内含子-外显子边界进行测序,以鉴定潜在的变体。采用最近建立的基于免疫组织化学的分类器来确定每个肿瘤的 CMS。
对来自卢旺达的 51 名患者的癌组织 DNA 进行测序分析,发现 23 名(45.1%)患者存在 TP53 致病性变异。这些变体主要是错义类型(18/23,78.3%)。最常见的是 c.455dup(p.P153Afs*28)、c.524G>A(p.R175H)和 c.733G>A(p.G245S),每个肿瘤均发现 3 个。对 23 个突变(其中 20 个为单碱基替换)的三核苷酸序列上下文分析显示,单碱基替换(SBS)中以 [C>N] 模式为主(18/20;90.0%),最常见的突变是 C[C>T]G(5/18,27.8%)。此外,嘧啶碱基(C 和 T)优先出现在突变胞嘧啶的 5'侧翼位置(13/18;72.2%)。对 CMS 亚型的分析显示以下分布:CMS1(微卫星不稳定-免疫)(6/51,11.8%)、CMS2(经典)(28/51,54.9%)、CMS3(代谢)(9/51,17.6%)和 CMS4(间质)(8/51,15.7%)。有趣的是,大多数 TP53 变体都存在于 CMS2 亚组中(14/23;60.1%)。
我们的研究结果表明,卢旺达 CRC 患者中存在高频的 TP53 变体。重要的是,这些变体在 CMS2 亚型中富集。本研究代表了对卢旺达 CRC 患者分子改变的第二次研究,也是首次探索 TP53 突变和 CMS 分类,为深入研究这一人群的 CRC 分子特征提供了有价值的见解。