Ozaki Tomohiko, Hiramatsu Masafumi, Nakamura Hajime, Niimi Yasunari, Tanoue Shuichi, Mizutani Katsuhiro, Nakahara Ichiro, Matsumaru Yuji, Matsumoto Yasushi, Krings Timo, Fujinaka Toshiyuki
Department of Neurosurgery, National Hospital Organization, Osaka National Hospital, 2-1-14 Hoenzaka, Chuo-ku, Osaka, 540-0006, Japan.
Department of Neurosurgery, Osaka University Graduate School of Medicine, Suita, Japan.
Neuroradiology. 2025 Jan;67(1):213-225. doi: 10.1007/s00234-024-03478-w. Epub 2024 Oct 12.
This study aimed to classify medullary bridging vein-draining dural arteriovenous fistulas (MBV-DAVFs) located around the foramen magnum (FM) according to their location and characterize their angioarchitecture and treatment outcomes.
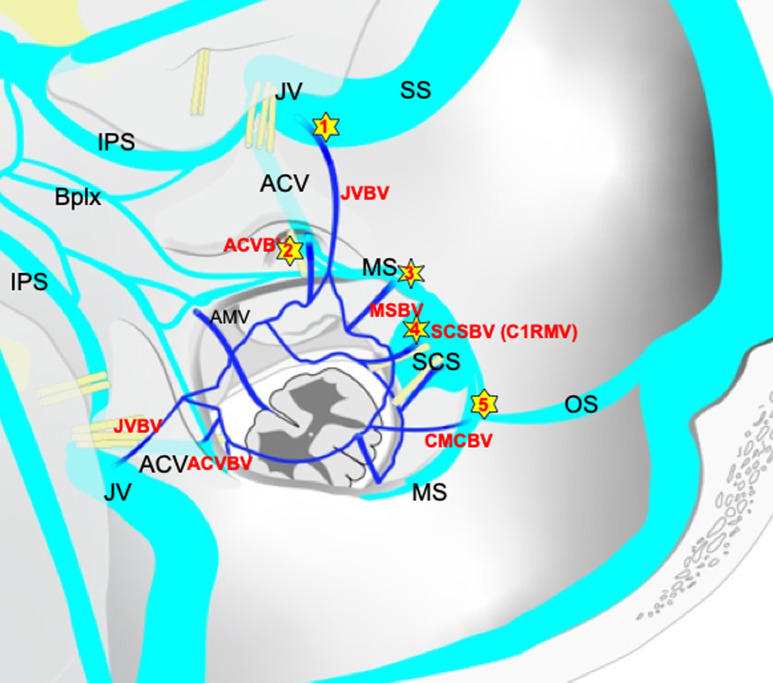
Patients with MBV-DAVFs diagnosed between January 2013 and October 2022 were included. MBV-DAVFs were classified into four groups. Jugular vein-bridging vein (JV-BV) DAVF: located in proximity to jugular fossa, Anterior condylar vein (ACV)-BV DAVF: proximity to anterior condylar canal, Marginal sinus (MS)-BV DAVF: lateral surface of FM and Suboccipital cavernous sinus (SCS)-BV DAVF: proximity to dural penetration of vertebral artery.
Twenty patients were included, three JV-BV, four ACV-BV, three MS-BV and ten SCS-BV DAVFs, respectively. All groups showed male predominance. There were significant differences in main feeders between JV (jugular branch of ascending pharyngeal artery) and SCS group (C1 dural branch). Pial feeders from anterior spinal artery (ASA) or lateral spinal artery (LSA) were visualized in four SCS and one MS group. Drainage pattern did not differ between groups. Transarterial embolization (TAE) was performed in three, two, one and two cases and complete obliteration was obtained in 100%, 50%, 100% and 0% in JV, ACS, MS and SCS group, respectively. Successful interventions without major complications were finally obtained in 100%, 75%, 100%, and 40% in JV, ACS, MS and SCS group, respectively.
JV-BV DAVFs were successfully treated using TAE alone. SCS-BV DAVFs were mainly fed by small C1 dural branches of vertebral artery often with pial feeders from ASA or LSA, and difficultly treated by TAE alone.
本研究旨在根据枕骨大孔(FM)周围的髓质桥静脉引流硬脑膜动静脉瘘(MBV-DAVF)的位置进行分类,并描述其血管构筑和治疗结果。
纳入2013年1月至2022年10月期间诊断为MBV-DAVF的患者。MBV-DAVF分为四组。颈静脉-桥静脉(JV-BV)DAVF:位于颈静脉窝附近;髁前静脉(ACV)-BV DAVF:靠近髁前管;边缘窦(MS)-BV DAVF:枕骨大孔外侧表面;枕下海绵窦(SCS)-BV DAVF:靠近椎动脉硬膜穿入处。
共纳入20例患者,分别为3例JV-BV、4例ACV-BV、3例MS-BV和10例SCS-BV DAVF。所有组均以男性为主。JV组(咽升动脉颈静脉支)和SCS组(C1硬膜支)的主要供血动脉存在显著差异。在4例SCS组和1例MS组中可见来自脊髓前动脉(ASA)或脊髓外侧动脉(LSA)的软膜供血动脉。各组之间的引流模式无差异。分别对3例、2例、1例和2例患者进行了经动脉栓塞(TAE),JV组、ACS组、MS组和SCS组的完全闭塞率分别为100%、50%、100%和0%。JV组、ACS组、MS组和SCS组最终成功干预且无重大并发症的比例分别为100%、75%、100%和40%。
JV-BV DAVF单独使用TAE即可成功治疗。SCS-BV DAVF主要由椎动脉的小C1硬膜支供血,常伴有来自ASA或LSA的软膜供血动脉,单独使用TAE治疗困难。