Munro Vicki, Mustafa Syed, Siddiqi Ferhan S, Rajaraman Murali, Costa Andreu F, Imran Syed Ali
Division of Endocrinology, Department of Medicine, Dalhousie University, 7N Victoria Building, 1276 South Park St Halifax, Halifax, NS, B3H 2Y9, Canada.
Faculty of Medicine, Dalhousie University, Halifax, NS, Canada.
Thyroid Res. 2024 Oct 14;17(1):23. doi: 10.1186/s13044-024-00213-8.
Differentiated thyroid cancer (DTC) requires long-term follow-up due to the risk of delayed recurrence. Follow-up surveillance involves serial neck ultrasound (US) and thyroglobulin (Tg); however, the optimal frequency and diagnostic performance of neck US outside of specialized thyroid cancer centres in higher risk patients is not well defined. We sought to evaluate the diagnostic performance of US and serial Tg in advanced stage DTC.
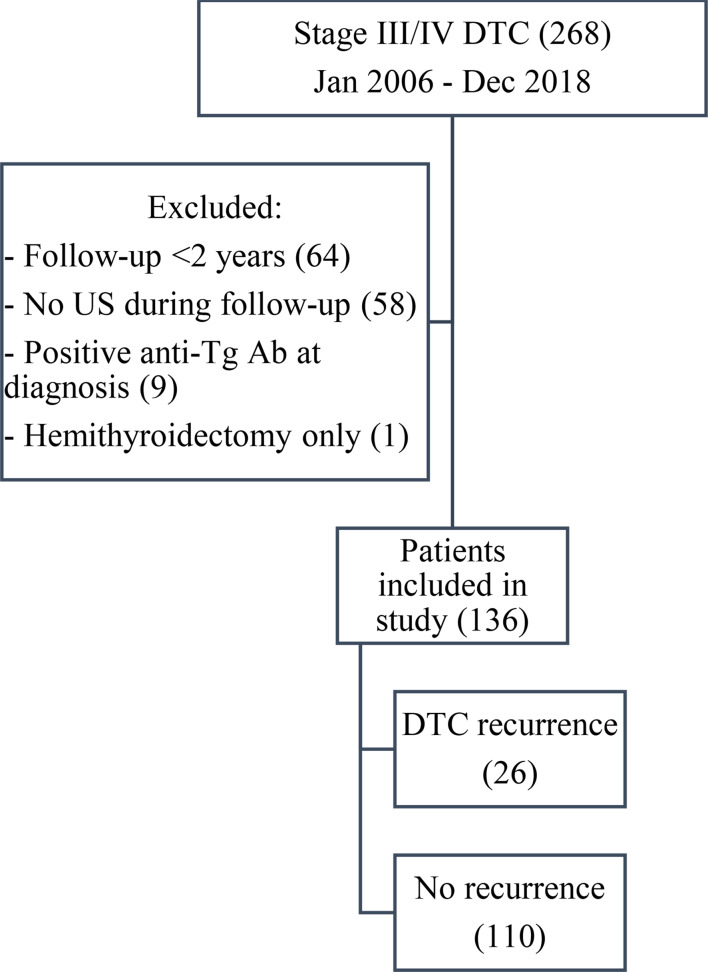
We retrospectively reviewed our thyroid cancer database for patients with stage III and IV DTC from 2006 to 2018, total thyroidectomy, and at least 2 years follow-up to assess recurrence rates. Those with hemi-thyroidectomy or anti-Tg antibodies were excluded. Diagnostic performance of US and Tg were assessed using a composite reference standard of follow-up imaging and pathology. All relevant US were reviewed by a blinded expert radiologist for uniformity.
Of 136 included patients (91 females, mean age 58.9), 26 (19%) had recurrence of DTC over median follow-up of 6.6 years (IQR 5.3-9.3). The sensitivity and specificity of US in diagnosing cervical recurrence were 73.3% (95% CI 0.51-0.96) and 68.3% (95% CI 0.60-0.77) based on historical reports, respectively, and 80% (95% CI 0.60-1.00) and 87.8% (95% CI 0.82-0.93) based on blinded expert review, respectively. Tg had a sensitivity of 95.5% (95% CI 0.89-1.0) and specificity of 96.2% (95% CI 0.92-0.99) in detecting cervical recurrence or distant metastases. False positive US findings on historical US and subsequent review occurred in 38 (28%) and 15 (11%) patients, respectively, while 5 (3.6%) had false positive Tg results.
Serial Tg has better sensitivity and specificity than US for detecting recurrence of advanced stage DTC. Furthermore, re-interpretation of abnormal findings using structured US reporting with a subspecialized reader may improve diagnostic performance of US and improve its utility in clinical care.
分化型甲状腺癌(DTC)由于存在延迟复发风险,需要长期随访。随访监测包括系列颈部超声(US)和甲状腺球蛋白(Tg);然而,在高风险患者中,非专业甲状腺癌中心颈部超声的最佳频率和诊断性能尚未明确界定。我们旨在评估超声和系列Tg在晚期DTC中的诊断性能。
我们回顾性分析了2006年至2018年期间III期和IV期DTC患者的甲状腺癌数据库,这些患者均接受了甲状腺全切术,且随访至少2年以评估复发率。排除接受半甲状腺切除术或存在抗Tg抗体的患者。使用随访成像和病理学的综合参考标准评估超声和Tg的诊断性能。所有相关超声均由一位不知情的专家放射科医生进行统一审查。
在纳入的136例患者(91例女性,平均年龄58.9岁)中,26例(19%)在中位随访6.6年(IQR 5.3 - 9.3)期间出现DTC复发。根据既往报告,超声诊断颈部复发的敏感性和特异性分别为73.3%(95%CI 0.51 - 0.96)和68.3%(95%CI 0.60 - 0.77),而根据不知情专家审查分别为80%(95%CI 0.60 - 1.00)和87.8%(95%CI 0.82 - 0.93)。Tg检测颈部复发或远处转移的敏感性为95.5%(95%CI 0.89 - 1.0),特异性为96.2%(95%CI 0.92 - 0.99)。既往超声检查和后续审查中超声的假阳性结果分别出现在38例(28%)和15例(11%)患者中,而5例(3.6%)有Tg假阳性结果。
系列Tg在检测晚期DTC复发方面比超声具有更好的敏感性和特异性。此外,使用结构化超声报告并由专科医生对异常结果进行重新解读,可能会提高超声的诊断性能及其在临床护理中的效用。