McArdle Ryan Patrick, Phru Ching Swe, Hossain Mohammad Sharif, Alam Mohammad Shafiul, Haldar Kasturi
Boler-Parseghian Center, Department of Biological Sciences, University of Notre Dame, USA.
Infectious Diseases Division, International Center for Diarrheal Disease Research, Bangladesh.
Lancet Reg Health Southeast Asia. 2024 Sep 27;31:100487. doi: 10.1016/j.lansea.2024.100487. eCollection 2024 Dec.
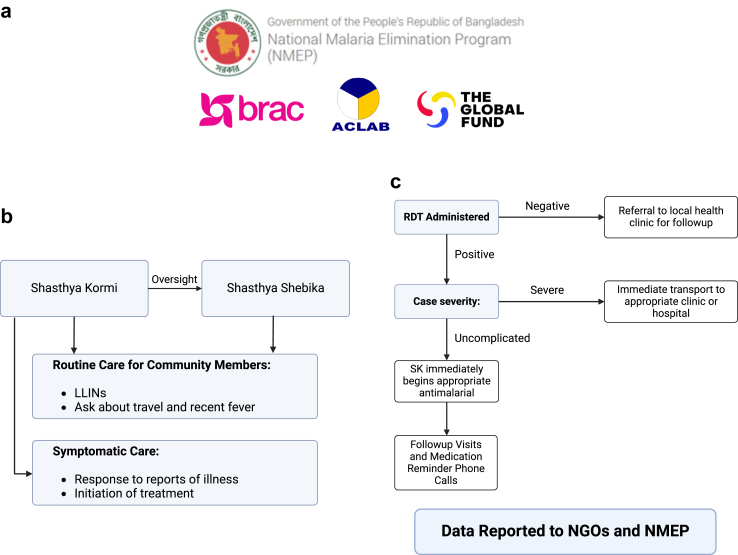
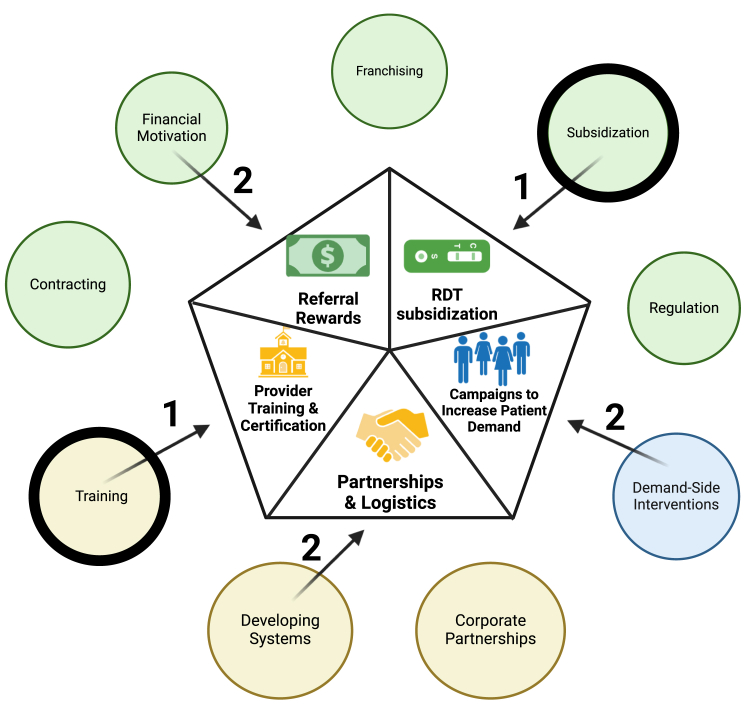
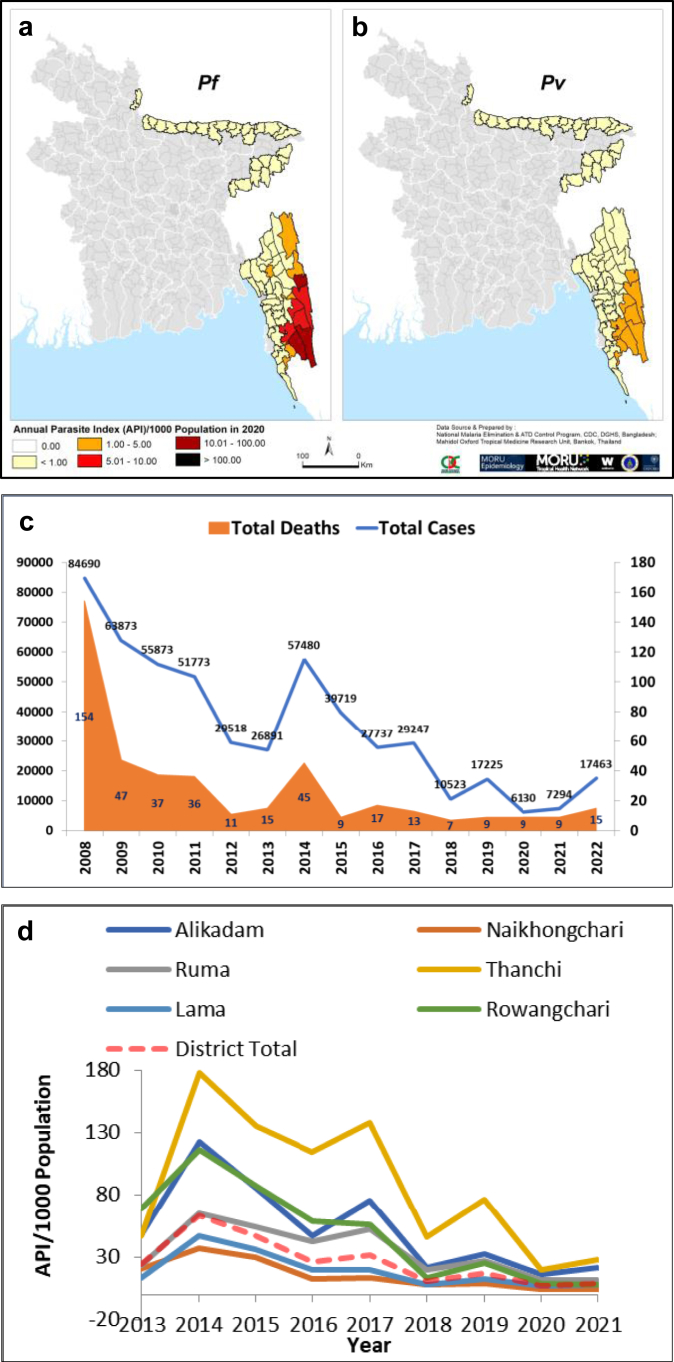
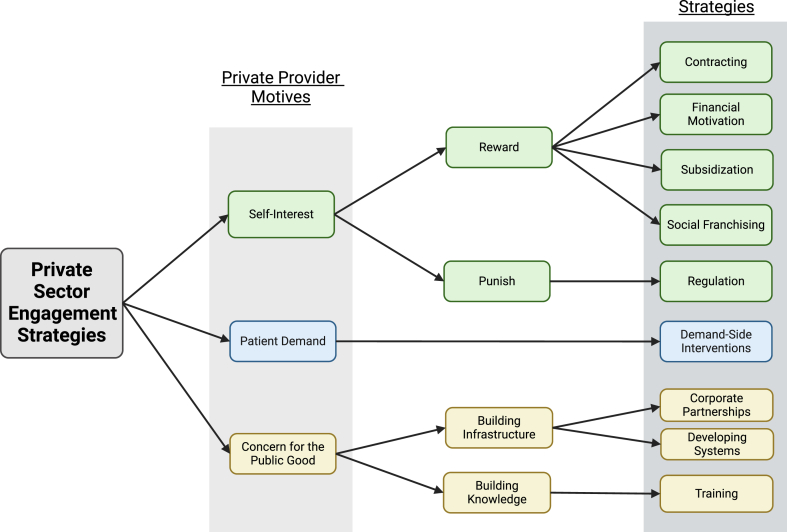
Bangladesh reduced malaria incidence by 93% from 2008 to 2020 through the action of governmental and non-governmental organizations. The Bangladesh context is unique to South Asia because its successful public sector malaria control programs have historically not engaged corporate partners (as undertaken in Sri Lanka and proposed in India). However, ∼18 million people continue to live at risk of infection in Bangladesh and for-profit private healthcare providers, catalytic for malaria elimination in many countries, are expected to benefit the national program. We distilled (from a large and complex literature) nine distinct strategies important in other developing settings and weighed them in the context of Bangladesh's flourishing private health care sector, driven by patient demand, self-interest and aspirations for public good, as well as heterogeneity in providers and malaria-prevalence. We propose a new model dependent on five strategies and its immediate deployment considerations in high endemic areas, to empower Bangladesh's phased agenda of eliminating indigenous malaria transmission by 2030.
通过政府和非政府组织的行动,孟加拉国在2008年至2020年间将疟疾发病率降低了93%。孟加拉国的情况在南亚是独特的,因为其成功的公共部门疟疾控制项目历来没有与企业合作伙伴合作(如斯里兰卡那样,印度也有此提议)。然而,在孟加拉国仍有大约1800万人面临感染风险,而在许多国家对消除疟疾起到催化作用的营利性私立医疗服务提供者,有望使国家项目受益。我们(从大量复杂的文献中)提炼出在其他发展环境中重要的九种不同策略,并在孟加拉国蓬勃发展的私立医疗保健部门的背景下权衡这些策略,该部门受患者需求、自身利益和公益愿望以及提供者和疟疾流行程度的异质性驱动。我们提出了一个依赖于五种策略的新模式及其在高流行地区的立即部署考虑因素,以推动孟加拉国到2030年消除本土疟疾传播的分阶段议程。