Wang Ya-Zhou, Peng Mao-Zhen, Xu Yao-Lin, Ying Ying, Tang Lin-Hui, Xu Hua-Xiang, He Jun-Yi, Liu Liang, Wang Wen-Quan
Department of Pancreatic Surgery, Zhongshan Hospital, Fudan University, 180 Feng Lin Road, Shanghai, 200032, China.
Cancer Center, Zhongshan Hospital, Fudan University, Shanghai, 200032, China.
Discov Oncol. 2024 Oct 15;15(1):560. doi: 10.1007/s12672-024-01420-3.
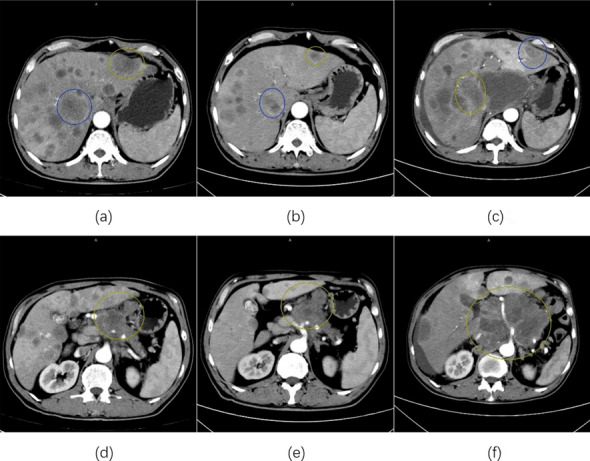
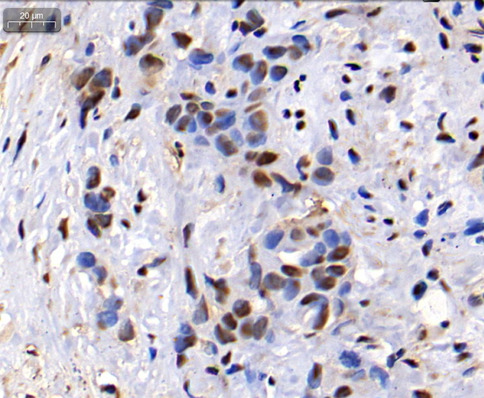
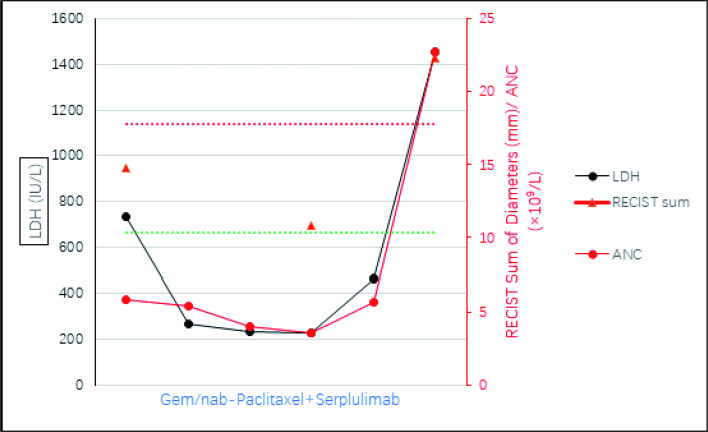
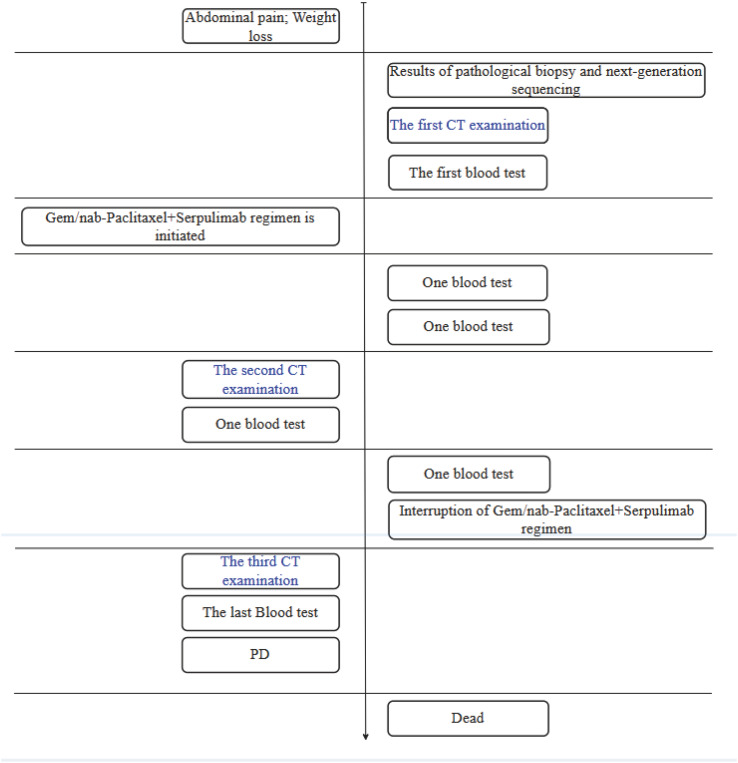
Pancreatic cancer is among the most immune-resistant tumor types due to its unique tumor microenvironment and low cancer immunogenicity. Single-agent immune modulators have thus far proven clinically ineffective. However, a growing body of evidence suggests that combination of these modulators with other strategies could unlock the potential of immunotherapy in pancreatic cancer. Herein, we describe the case of a 59-year-old male with metastatic pancreatic ductal adenocarcinoma, referred to our center to receive immunotherapy (serplulimab, a novel anti-PD-1 antibody) combined with chemotherapy (gemcitabine/nab-paclitaxel). During the initial three treatment cycles, the patient was assessed as having stable disease (SD) according to RECIST 1.1 criteria. However, following two additional cycles of combination therapy, the primary tumor mass increased from 4.9 cm to 13.2 cm, accompanied by the development of new lung lesions, ascites, and pelvic metastases. He succumbed to respiratory failure one month later. Retrospective analysis revealed that the patient had MDM4 amplification, identified as a high-risk factor for hyperprogressive disease (HPD). To our knowledge, this is the first reported case of HPD in pancreatic cancer with multiple metastases treated using combination therapy. We investigated the potential mechanisms and reviewed the latest literature on predictive factors for HPD. These findings suggest that while chemotherapy combined with immunotherapy may hold promise for treating pancreatic cancer, it is imperative to identify and closely monitor patients with high-risk factors for HPD when using immunotherapy.
由于其独特的肿瘤微环境和低癌症免疫原性,胰腺癌是免疫抵抗性最强的肿瘤类型之一。单药免疫调节剂迄今为止在临床上已被证明无效。然而,越来越多的证据表明,将这些调节剂与其他策略联合使用可能会释放免疫疗法在胰腺癌治疗中的潜力。在此,我们描述了一名59岁男性转移性胰腺导管腺癌患者的病例,该患者转诊至我们中心接受免疫治疗(斯鲁利单抗,一种新型抗PD-1抗体)联合化疗(吉西他滨/白蛋白结合型紫杉醇)。在最初的三个治疗周期中,根据RECIST 1.1标准评估患者疾病稳定(SD)。然而,在额外两个周期的联合治疗后,原发肿瘤肿块从4.9厘米增加到13.2厘米,同时出现了新的肺部病变、腹水和盆腔转移。一个月后,他死于呼吸衰竭。回顾性分析显示,该患者存在MDM4扩增,这被确定为超进展性疾病(HPD)的高危因素。据我们所知,这是首例使用联合疗法治疗的多发转移胰腺癌HPD病例报告。我们研究了潜在机制,并回顾了关于HPD预测因素的最新文献。这些发现表明,虽然化疗联合免疫疗法可能有望治疗胰腺癌,但在使用免疫疗法时,识别并密切监测具有HPD高危因素的患者至关重要。