Castelli Sveva, Thorwarth Anne, van Schewick Claudia, Wendt Anke, Astrahantseff Kathy, Szymansky Annabell, Lodrini Marco, Veldhoen Simon, Gratopp Alexander, Mall Marcus A, Eggert Angelika, Deubzer Hedwig E
Department of Pediatric Oncology and Hematology, Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Campus Virchow Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany.
Department of Pediatric Respiratory Medicine, Immunology and Critical Care Medicine, Charité-Universitätsmedizin Berlin, Campus Virchow Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany.
J Clin Med. 2024 Oct 8;13(19):5995. doi: 10.3390/jcm13195995.
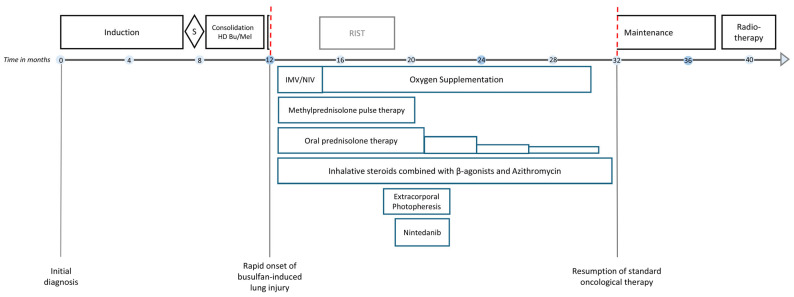
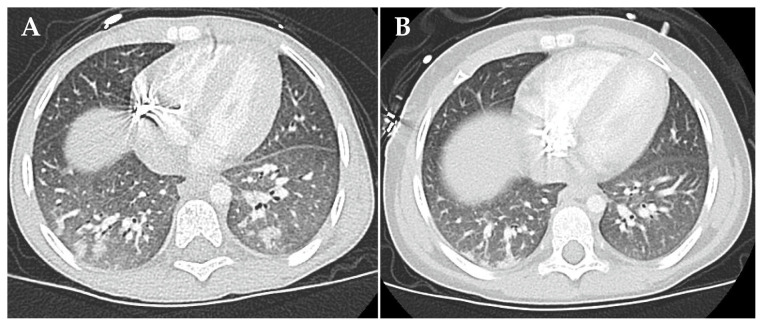
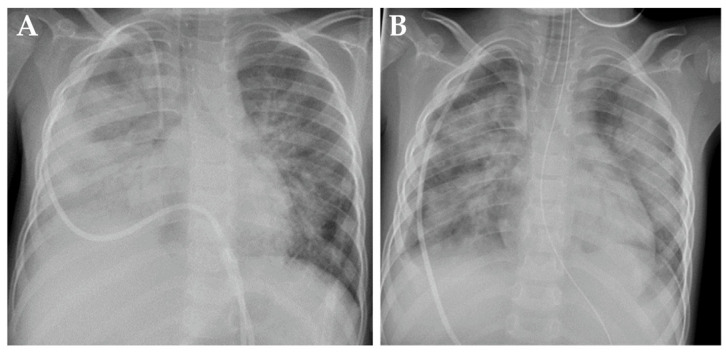
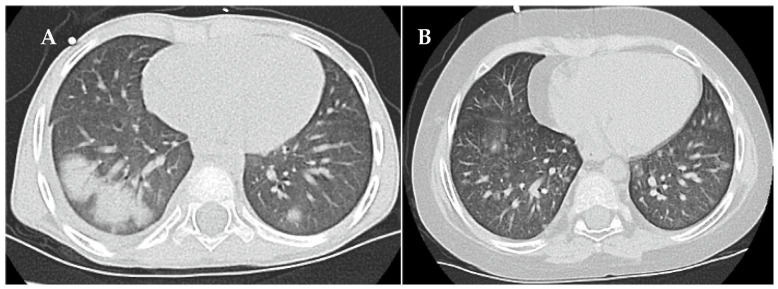
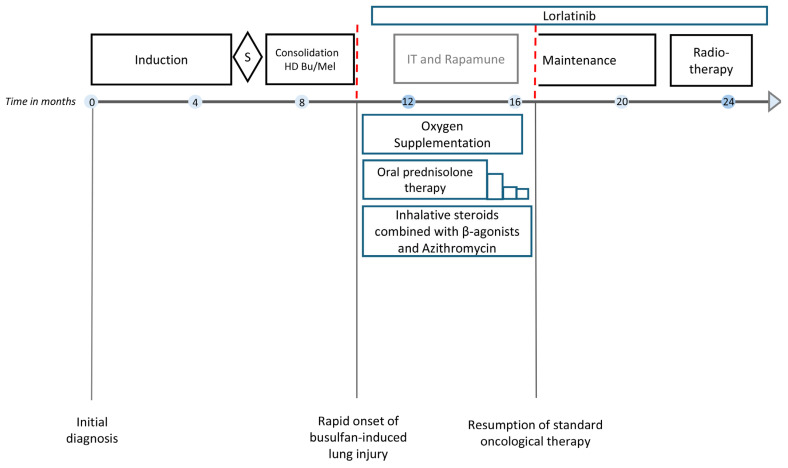
: Integrating the cytotoxic drug busulfan into a high-dose chemotherapy regimen prior to autologous hematopoietic stem cell rescue in patients with high-risk neuroblastoma has improved the survival of children battling this deadly disease. Busulfan-induced toxicities can, however, be severe. Here, we describe the diagnosis and successful treatment of acute pulmonary injury by total-body-weight-adjusted busulfan therapy in two children with high-risk neuroblastoma. : Patient 1 developed life-threatening biphasic acute respiratory failure on days +60 and +100 after busulfan therapy, requiring intubation and invasive mechanical ventilation. Despite intensive anti-inflammatory and immunomodulatory therapy, including systemic corticosteroids, topical inhalation regimens, azithromycin, nintedanib and extracorporal photopheresis, patient 1 required extended intensive care measures and non-invasive respiratory support for a total of 20 months. High-resolution computed tomography showed diffuse intra-alveolar and interstitial patterns. Patient 2 developed partial respiratory failure with insufficient oxygen saturation and dyspnea on day +52 after busulfan therapy. Symptoms were resolved after 6 months of systemic corticosteroids, topical inhalation regimens and azithromycin. High-resolution computed tomography showed atypical pneumonic changes with ground-glass opacities. While both patients fully recovered without evidence of pulmonary fibrosis, cancer therapy had to be paused and then modified until full recovery from busulfan-induced lung injury. : Busulfan-induced lung injury requires prompt diagnosis and intervention. Symptoms and signs are nonspecific and difficult to differentiate from other causes. Therapeutic busulfan drug level monitoring and the identification of patients at risk for drug overdosing through promoter polymorphisms in the glutathione S-transferase alpha 1 gene encoding the main enzyme in busulfan metabolism are expected to reduce the risk of busulfan-induced toxicities.
在高危神经母细胞瘤患者进行自体造血干细胞救援之前,将细胞毒性药物白消安纳入大剂量化疗方案可提高与这种致命疾病作斗争的儿童的生存率。然而,白消安引起的毒性可能很严重。在此,我们描述了两名高危神经母细胞瘤儿童因按总体重调整白消安治疗而导致的急性肺损伤的诊断和成功治疗。患者1在白消安治疗后第60天和第100天出现危及生命的双相性急性呼吸衰竭,需要插管和有创机械通气。尽管进行了强化抗炎和免疫调节治疗,包括全身用皮质类固醇、局部吸入方案、阿奇霉素、尼达尼布和体外光化学疗法,患者1仍需要延长的重症监护措施和无创呼吸支持,总共持续了20个月。高分辨率计算机断层扫描显示弥漫性肺泡和间质模式。患者2在白消安治疗后第52天出现部分呼吸衰竭,血氧饱和度不足和呼吸困难。经过6个月的全身用皮质类固醇、局部吸入方案和阿奇霉素治疗后症状得到缓解。高分辨率计算机断层扫描显示非典型肺炎改变伴磨玻璃影。虽然两名患者均完全康复且无肺纤维化迹象,但癌症治疗不得不暂停,然后进行调整,直到从白消安引起的肺损伤中完全康复。白消安引起的肺损伤需要及时诊断和干预。症状和体征是非特异性的,难以与其他原因区分开来。治疗性白消安药物水平监测以及通过编码白消安代谢主要酶的谷胱甘肽S-转移酶α1基因中的启动子多态性来识别药物过量风险患者,有望降低白消安引起的毒性风险。