Burgmann Christian Herbert, Sachs Ulrich J, Trautmann-Grill Karolin, Pfrepper Christian, Knöbl Paul, Greil Richard, Oldenburg Johannes, Miesbach Wolfgang, Holstein Katharina, Eichler Hermann, Möhnle Patrick, Höpting Matthias, Dobbelstein Christiane, Klamroth Robert, Tiede Andreas
Hematology, Hemostasis, Oncology, and Stem Cell Transplantation, Hannover Medical School, Hannover, Germany.
Institute for Clinical Immunology and Transfusion Medicine, Justus Liebig University, Giessen, Germany.
Res Pract Thromb Haemost. 2024 Sep 5;8(7):102565. doi: 10.1016/j.rpth.2024.102565. eCollection 2024 Oct.
Persons with acquired hemophilia A are often older and suffer from comorbidity or frailty. Little is known about the impact on clinically relevant outcomes of acquired hemophilia A.
To assess the relevance of age, physical performance status, comorbidity, and concomitant medication on the risk of bleeding and other outcomes.
Post hoc analysis of data from the GTH-AHA-EMI study that used emicizumab for bleed protection and withheld immunosuppressive treatment during the early phase of management. Primary endpoint was the rate of clinically relevant new bleeding (CRNB) during the first 12 weeks of emicizumab prophylaxis.
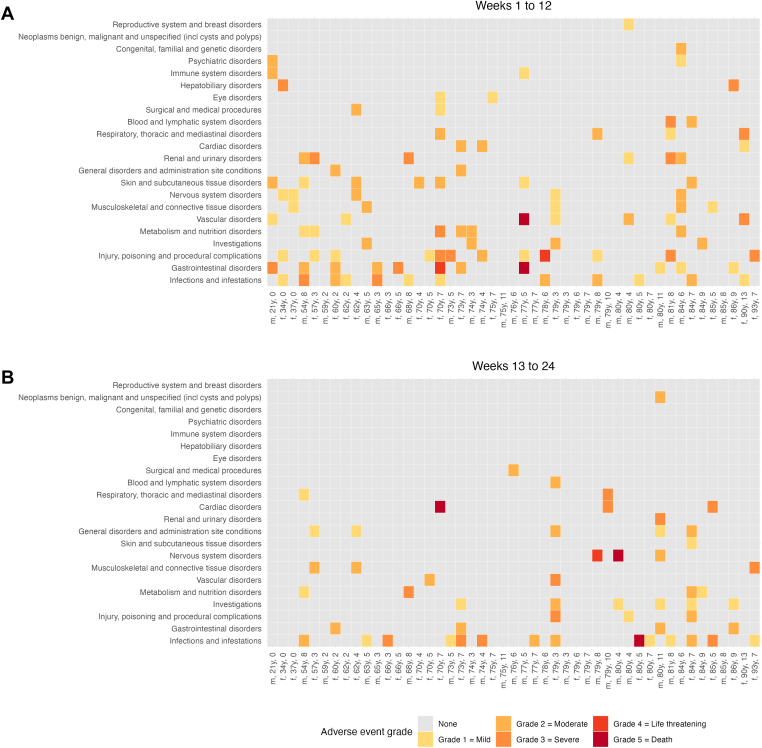
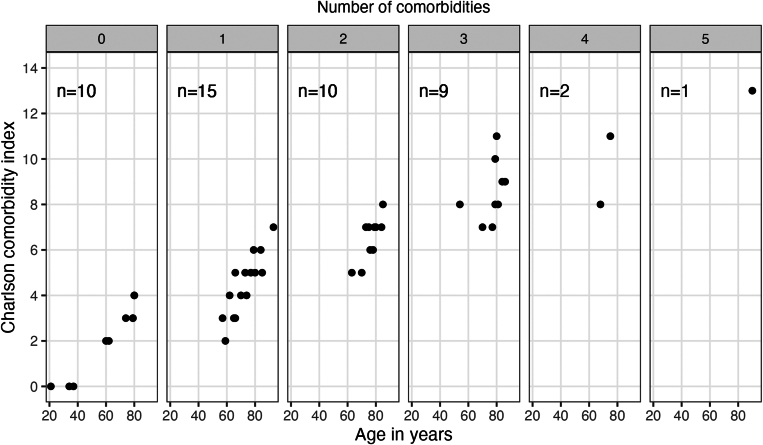
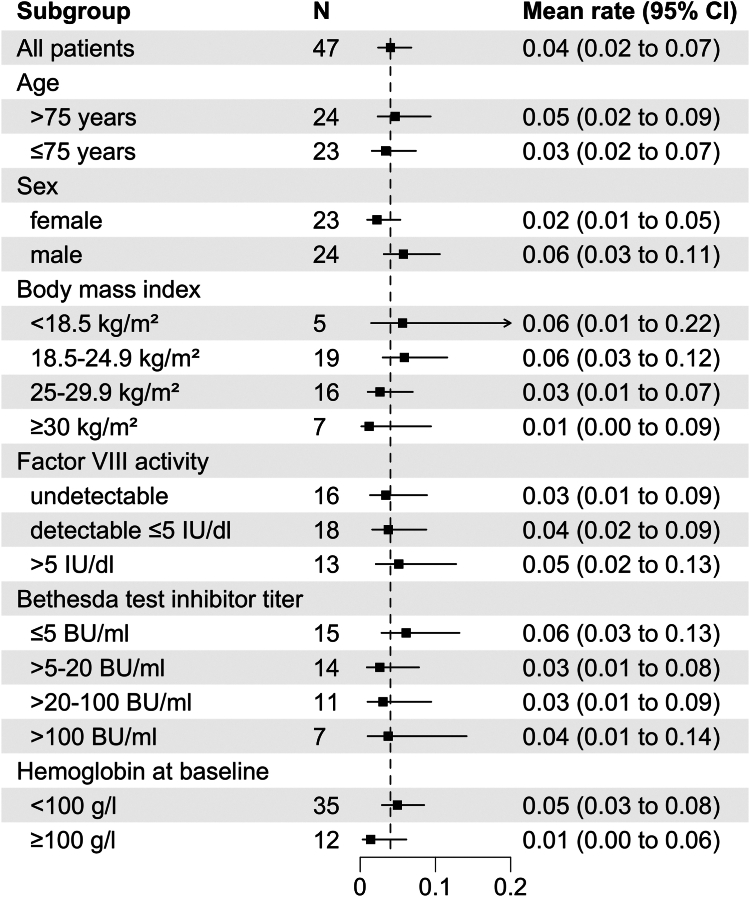
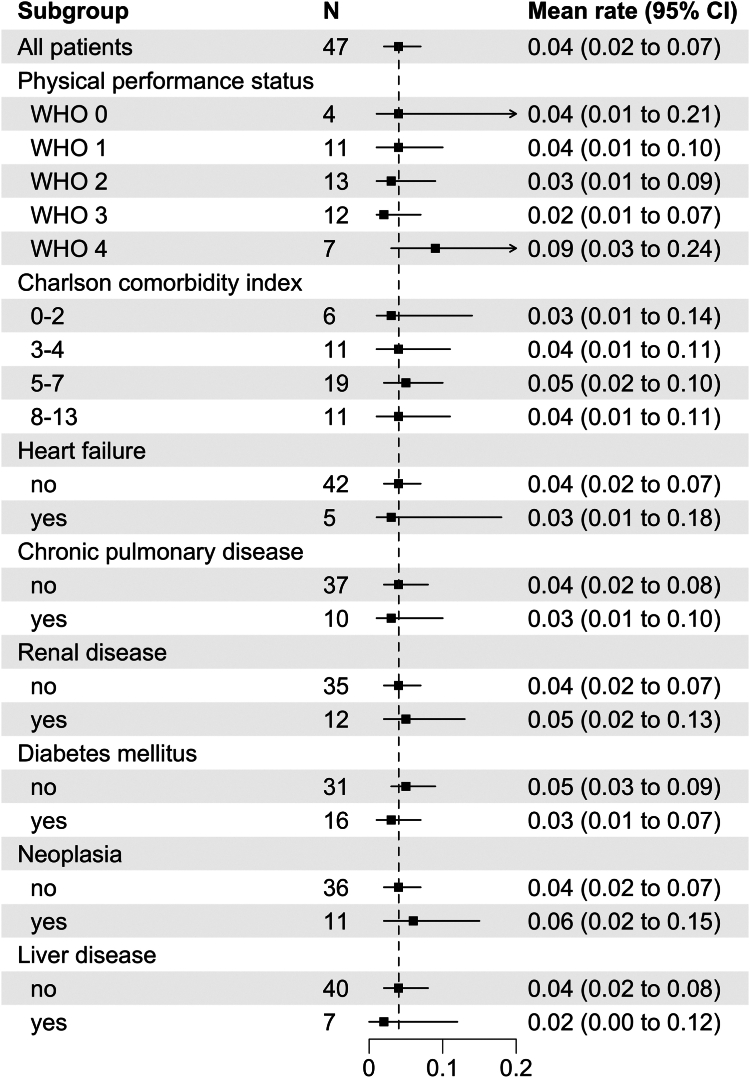
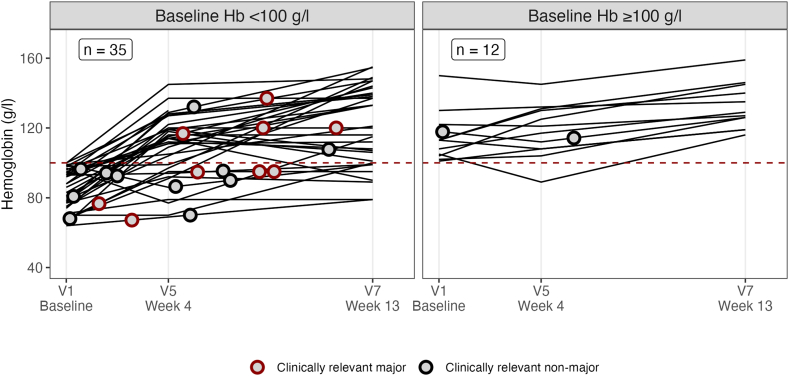
Forty-seven patients were enrolled. Median age was 76 years; performance status (World Health Organization performance status [WHO-PS]) was 3 or worse in 41%; Charlson comorbidity index (CCI) was 5 or higher in 63%; antithrombotic drugs were reported in 34%. Rate of CRNB during 12 weeks of emicizumab prophylaxis was similar across subgroups of age, sex, WHO-PS, CCI, baseline factor VIII activity, and inhibitor titer. Patients with CRNB during the study had more severe anemia already at baseline. However, persistent severe anemia in week 4 was not related to risk of bleeding beyond this time. CRNB was associated with injury from falling in 7 of 14 patients. Adverse events grade 3 or higher were not related to baseline CCI or age but were more frequent in patients with poor WHO-PS.
Emicizumab provided bleed protection regardless of age and comorbidity. Clinical baseline characteristics did not predict breakthrough bleeding under emicizumab. Poor WHO-PS at baseline was associated with severe adverse events during the study.
获得性血友病A患者通常年龄较大,且患有合并症或身体虚弱。关于获得性血友病A对临床相关结局的影响知之甚少。
评估年龄、身体功能状态、合并症和伴随用药对出血风险及其他结局的相关性。
对GTH-AHA-EMI研究的数据进行事后分析,该研究在管理早期使用艾美赛珠单抗预防出血并停用免疫抑制治疗。主要终点是艾美赛珠单抗预防的前12周内临床相关新出血(CRNB)率。
共纳入47例患者。中位年龄为76岁;41%的患者身体功能状态(世界卫生组织身体功能状态[WHO-PS])为3级或更差;63%的患者查尔森合并症指数(CCI)为5或更高;34%的患者报告使用了抗血栓药物。在年龄、性别、WHO-PS、CCI基线因子VIII活性和抑制剂滴度的亚组中,艾美赛珠单抗预防12周期间的CRNB率相似。研究期间发生CRNB的患者在基线时已有更严重的贫血。然而,第4周持续存在的严重贫血与此后的出血风险无关。14例患者中有7例的CRNB与跌倒损伤有关。3级或更高等级的不良事件与基线CCI或年龄无关,但在WHO-PS较差的患者中更常见。
无论年龄和合并症如何,艾美赛珠单抗均可提供出血保护。临床基线特征不能预测艾美赛珠单抗治疗下的突破性出血。基线WHO-PS较差与研究期间的严重不良事件有关。