, Data-Lead Africa, 10th street, Bassan Plaza, Block F, 3rd floor, Central Business District, Abuja, Nigeria.
Big Data Institute, Nuffield Department of Population Health, University of Oxford, Oxford, UK.
BMC Public Health. 2024 Oct 18;24(1):2882. doi: 10.1186/s12889-024-20378-z.
Childhood malnutrition is a complex issue with a range of contributing factors. The consequences of malnutrition are severe, particularly for children. This study aims to identify the factors contributing to inequality gaps in childhood malnutrition. Our study provides insights into modifiable elements to inform interventions targeted at distinct contexts and populations to improve child nutrition.
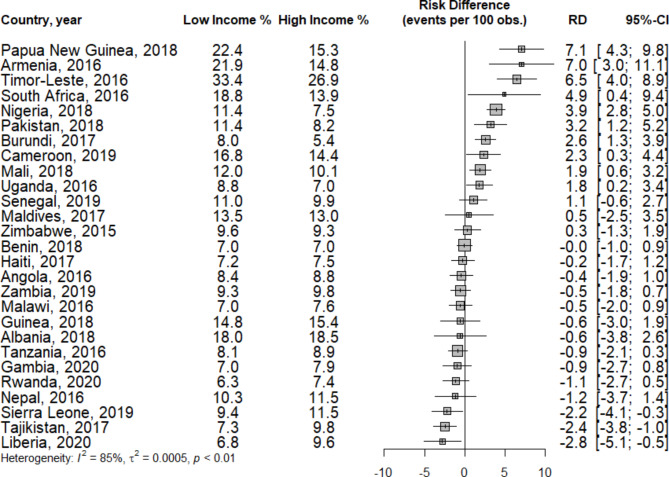
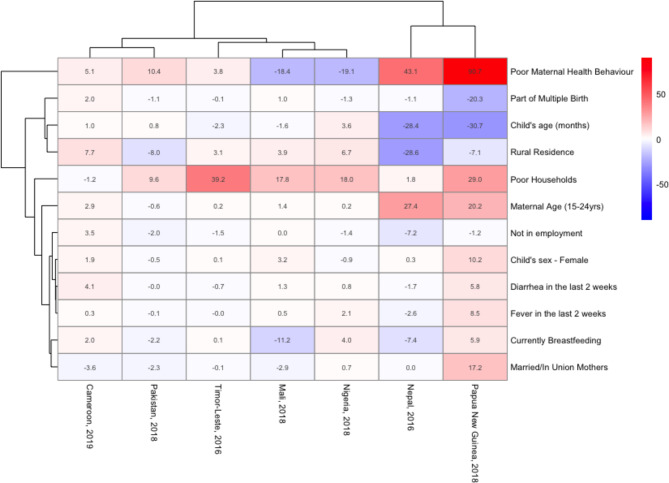
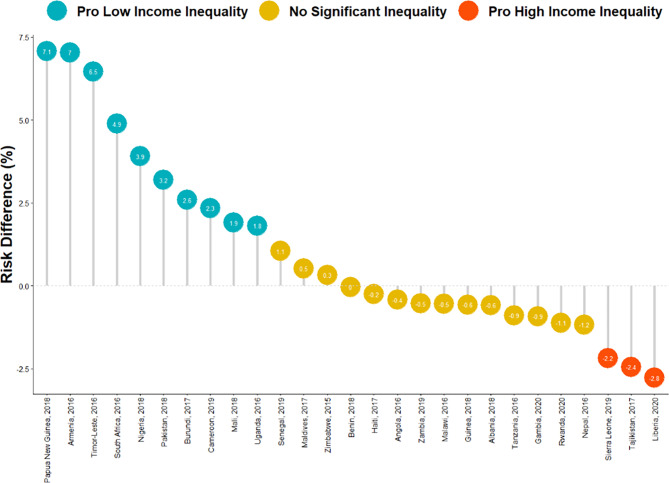
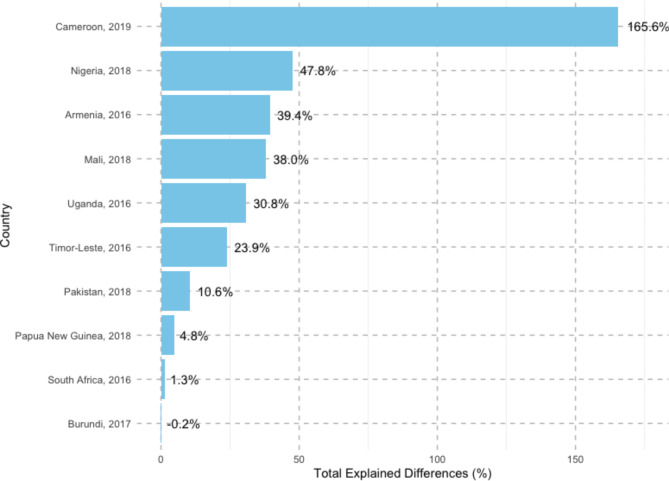
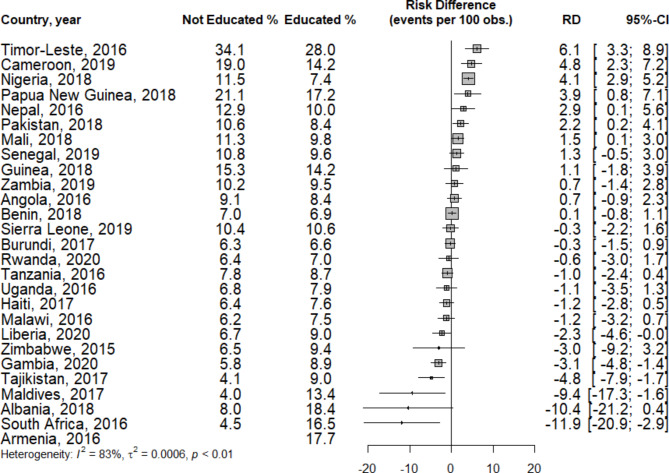
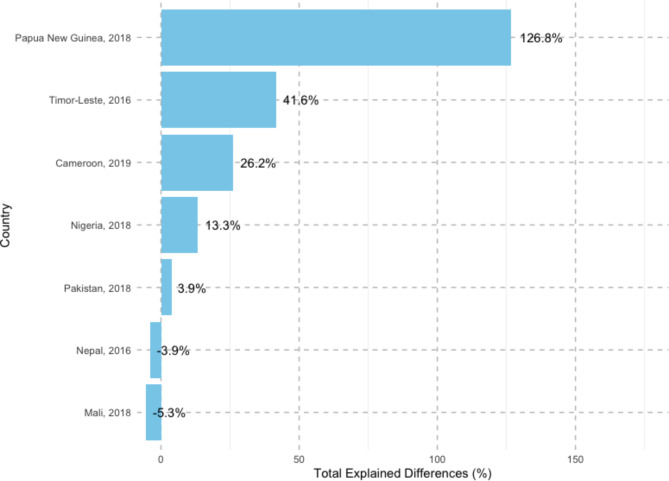
This study utilized data from the Demographic and Health Surveys (DHS) of 27 countries. First, the risk differences (RDs) between the prevalence of childhood malnutrition among the determinant variables, household income, and maternal education categories were calculated. The Blinder‒Oaxaca decomposition was subsequently used to determine the extent to which the difference in childhood malnutrition prevalence between low-income and high-income groups and maternal education levels results from the contributory effects of the explanatory variables: child and maternal individual-level compositional factors.
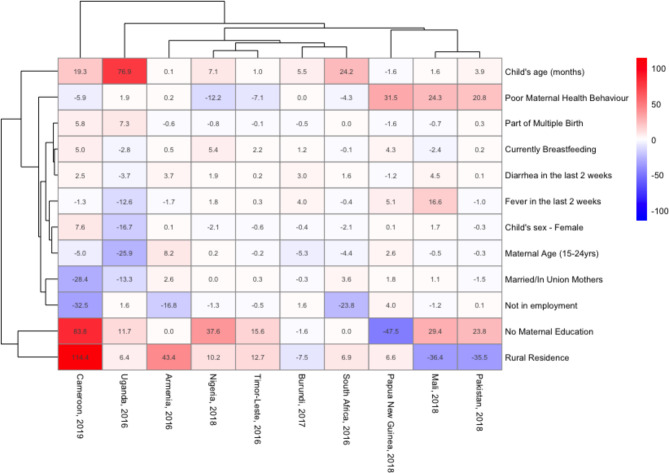
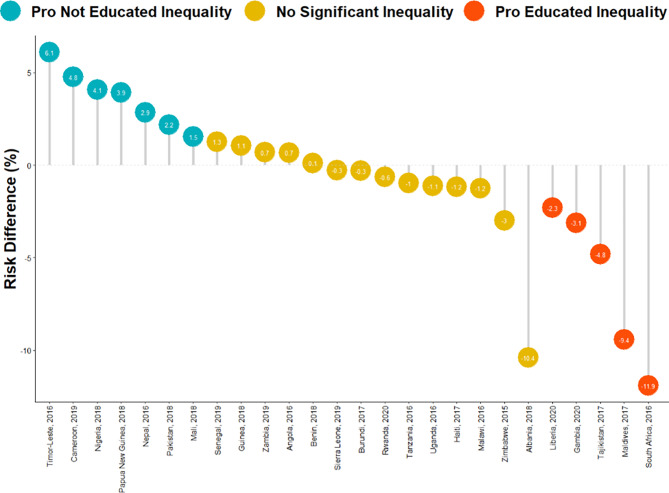
We examined data from 138,782 children in 27 countries from 2015 to 2020. The prevalence of childhood malnutrition (10.5%) varied across countries, ranging from 6.5% in Burundi to 29.5% in Timor Leste. On average, the prevalence of childhood malnutrition was 11.0% in low-income households and 10.7% among mothers without education. Some nations had pro-low-income (i.e., malnutrition concentrated among children from poor households) or pro-no-maternal education (i.e., malnutrition concentrated among children from mothers with no formal education) inequality in childhood malnutrition, but most did not. We found a complex interplay of compositional effects, such as the child's age, maternal education, maternal health behavior, and place of residence, that influence the inequality in childhood malnutrition rates across 10 pro-low-income countries. In addition, we also found that a complex mix of compositional effects, such as the household wealth index, maternal health behavior, and maternal age, contribute to childhood malnutrition inequality between educated and uneducated mothers across the 7 pro-no maternal education countries.
The prevalence of childhood malnutrition varies among low-income, high-income, and no maternal education-maternal education groups. This study highlights the need for a country-specific approach to addressing childhood malnutrition, with policies and interventions tailored to each country's specific context.
儿童营养不良是一个复杂的问题,有多种因素导致。营养不良的后果是严重的,特别是对儿童。本研究旨在确定导致儿童营养不良不平等差距的因素。我们的研究提供了可改变因素的见解,以便为不同的情况和人群提供干预措施,改善儿童营养。
本研究使用了来自 27 个国家的人口与健康调查(DHS)的数据。首先,计算了决定变量(家庭收入和母亲教育类别)之间儿童营养不良患病率的风险差异(RD)。随后,使用布伦纳-奥克萨卡分解法来确定在低收入和高收入群体以及母亲教育水平之间,儿童营养不良患病率的差异在多大程度上是由解释变量的贡献效应造成的:儿童和母亲个人层面的构成因素。
我们研究了 2015 年至 2020 年间来自 27 个国家的 138782 名儿童的数据。儿童营养不良的患病率(10.5%)在各国之间有所不同,从布隆迪的 6.5%到东帝汶的 29.5%不等。平均而言,低收入家庭的儿童营养不良患病率为 11.0%,没有受过教育的母亲的儿童营养不良患病率为 10.7%。一些国家的儿童营养不良存在亲低收入(即营养不良集中在贫困家庭的儿童中)或亲无母亲教育(即营养不良集中在没有接受过正规教育的母亲的儿童中)不平等现象,但大多数国家没有这种现象。我们发现,儿童年龄、母亲教育、母亲健康行为和居住地等构成因素的复杂相互作用影响了 10 个亲低收入国家的儿童营养不良率的不平等。此外,我们还发现,在 7 个亲无母亲教育的国家中,家庭财富指数、母亲健康行为和母亲年龄等构成因素的复杂组合导致了受过教育和未受过教育母亲的儿童营养不良不平等。
儿童营养不良的患病率在低收入、高收入和无母亲教育-母亲教育群体中有所不同。本研究强调了需要针对每个国家的具体情况采取具体的国家方法来解决儿童营养不良问题,制定适合每个国家具体情况的政策和干预措施。