Artz Mark E, Brooks Eric D
Department of Radiation Oncology, University of Florida College of Medicine, Jacksonville, FL, USA.
Premier Radiation Oncology Associates, Clearwater, FL, USA.
Int J Part Ther. 2024 Jun 20;14:100109. doi: 10.1016/j.ijpt.2024.100109. eCollection 2024 Dec.
To increase awareness of peri-radiation therapy (RT) intervention that may unduly heighten the risk of toxicity in lung cancer patients and encourage molecular testing and pretreatment consultation with rheumatology for patients with active autoimmune conditions.
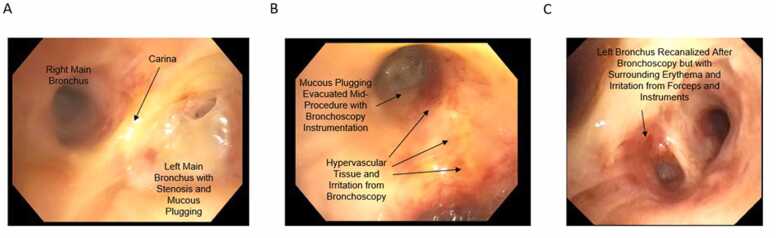
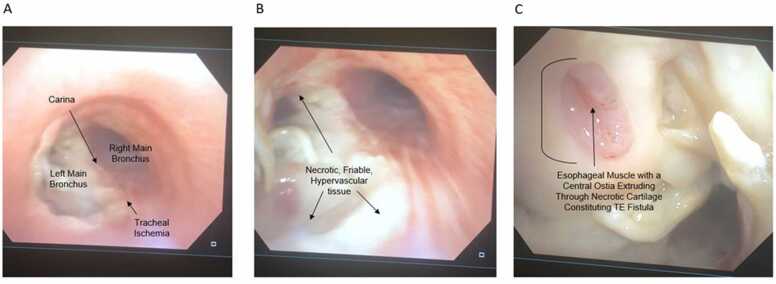
A 42-year-old male with an autoimmune disease was diagnosed with non-small cell lung cancer. He received 4 cycles of pemetrexed/cisplatin with proton therapy (PT) delivered halfway through for a bronchial stump positive margin. After completing the first cycle of adjuvant chemotherapy, he was given 61.6 Gy in 28 fractionations of PT. Before restarting chemotherapy, he experienced a dry cough and later shortness of breath (SOB), which resolved with an aggressive steroid taper. After completing his third cycle of cisplatin/pemetrexed, his SOB and cough worsened. He was admitted for an urgent bronchoscopy with debridement of the distal trachea and proximal left main bronchus. He received high-dose steroids again and another bronchoscopy, revealing a tracheoesophageal fistula. Rheumatology identified an MDA5+ and PL7-positive dermatomyositis subtype at this time, known to be associated with rare ulcerative symptoms.
A rare MDA5+ and PL7-positive dermatomyositis subtype, discovered post treatment, most likely contributed to SOB and cough following chemotherapy and PT, resulting in bronchoscopy of the irradiated field. A combination of these factors may have contributed to the tracheoesophageal fistula.
Patients with autoimmune disease should be carefully evaluated for rare underlying subtypes that could pose a danger to treatment. Oncologists should continue to be vigilant about underlying genetic predisposing factors that lead to exacerbated toxicity. Immunosuppressive agents given with RT may be considered for patients with autoimmune disease. Avoidance of biopsy, tissue manipulation, debridement, or any form of soft-tissue or hard-tissue violation needs to be discussed across the multidisciplinary spectrum to avoid nonhealing lesions shortly after RT.
提高对放疗(RT)期间干预措施的认识,这些干预措施可能会不适当地增加肺癌患者的毒性风险,并鼓励对患有活动性自身免疫性疾病的患者进行分子检测以及在放疗前咨询风湿病科。
一名患有自身免疫性疾病的42岁男性被诊断为非小细胞肺癌。他接受了4个周期的培美曲塞/顺铂化疗,并在疗程进行到一半时接受了质子治疗(PT),用于处理支气管残端切缘阳性情况。在完成第一个周期的辅助化疗后,他接受了28次分割的PT,总剂量为61.6 Gy。在重新开始化疗之前,他出现了干咳,随后出现气短(SOB),通过积极减少类固醇用量后症状缓解。在完成第三个周期的顺铂/培美曲塞化疗后,他的气短和咳嗽症状加重。他因紧急支气管镜检查入院,对远端气管和左主支气管近端进行清创。他再次接受了高剂量类固醇治疗,并进行了另一次支气管镜检查,发现了气管食管瘘。此时,风湿病科确定其为MDA5+和PL7阳性的皮肌炎亚型,已知该亚型与罕见的溃疡性症状相关。
治疗后发现的一种罕见的MDA5+和PL7阳性皮肌炎亚型,很可能是化疗和PT后出现气短和咳嗽的原因,导致了对放疗区域进行支气管镜检查。这些因素的综合作用可能导致了气管食管瘘。
对于自身免疫性疾病患者,应仔细评估是否存在可能对治疗构成危险的罕见潜在亚型。肿瘤学家应继续警惕导致毒性加剧的潜在遗传易感性因素。对于自身免疫性疾病患者,可考虑在放疗时使用免疫抑制剂。需要在多学科范围内讨论避免活检、组织操作、清创或任何形式的软组织或硬组织损伤,以避免放疗后不久出现不愈合的病变。